

Microvascular and Cardiovascular Outcomes According to Renal Function in Patients Treated With Once-Weekly Exenatide: Insights From the EXSCEL Trial
- PMID: 31757838
- PMCID: PMC7411285
- DOI: 10.2337/dc19-1065
Microvascular and Cardiovascular Outcomes According to Renal Function in Patients Treated With Once-Weekly Exenatide: Insights From the EXSCEL Trial
Abstract
Objective: To evaluate the impact of once-weekly exenatide (EQW) on microvascular and cardiovascular (CV) outcomes by baseline renal function in the Exenatide Study of Cardiovascular Event Lowering (EXSCEL).
Research design and methods: Least squares mean difference (LSMD) in estimated glomerular filtration rate (eGFR) from baseline between the EQW and placebo groups was calculated for 13,844 participants. Cox regression models were used to estimate effects by group on incident macroalbuminuria, retinopathy, and major adverse CV events (MACE). Interval-censored time-to-event models estimated effects on renal composite 1 (40% eGFR decline, renal replacement, or renal death) and renal composite 2 (composite 1 variables plus macroalbuminuria).
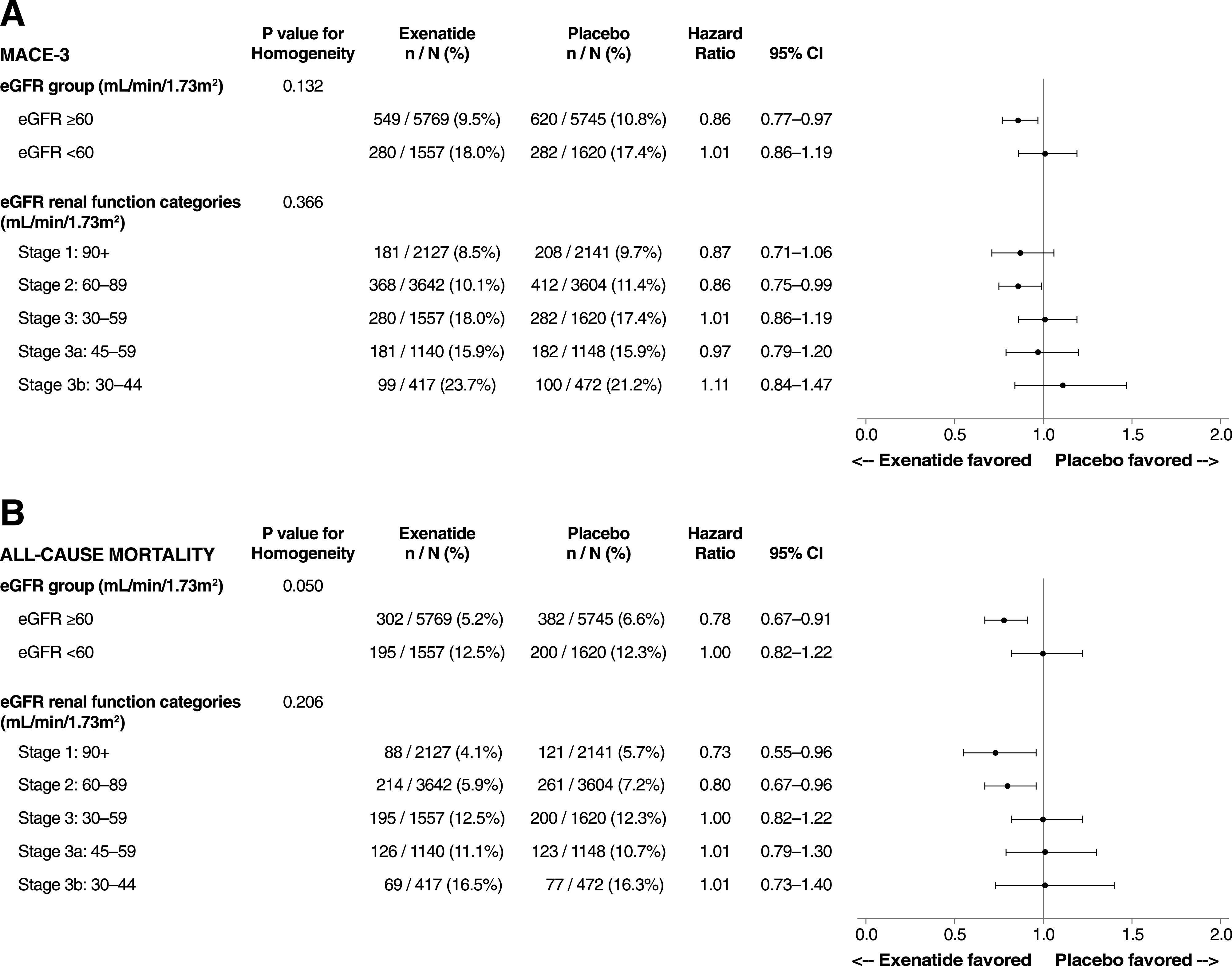
Results: EQW did not change eGFR significantly (LSMD 0.21 mL/min/1.73 m2 [95% CI -0.27 to 0.70]). Macroalbuminuria occurred in 2.2% of patients in the EQW group and in 2.5% of those in the placebo group (hazard ratio [HR] 0.87 [95% CI 0.70-1.07]). Neither renal composite was reduced with EQW in unadjusted analyses, but renal composite 2 was reduced after adjustment (HR 0.85 [95% CI 0.74-0.98]). Retinopathy rates did not differ by treatment group or in the HbA1c-lowering or prior retinopathy subgroups. CV outcomes in those with eGFR <60 mL/min/1.73 m2 did not differ by group. Those with eGFR ≥60 mL/min/1.73 m2 had nominal risk reductions for MACE, all-cause mortality, and CV death, but interactions by renal function group were significant for only stroke (HR 0.74 [95% CI 0.58-0.93]; P for interaction = 0.035) and CV death (HR 1.08 [95% CI 0.85-1.38]; P for interaction = 0.031).
Conclusions: EQW had no impact on unadjusted retinopathy or renal outcomes. CV risk was modestly reduced only in those with eGFR ≥60 mL/min/1.73 m2 in analyses unadjusted for multiplicity.
© 2019 by the American Diabetes Association.
Figures
References
-
- So WY, Kong AP, Ma RC, et al. . Glomerular filtration rate, cardiorenal end points, and all-cause mortality in type 2 diabetic patients. Diabetes Care 2006;29:2046–2052 - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) [published correction appears in Lancet 1999;354:602] Lancet 1998;352:837–853 - PubMed
-
- Turnbull FM, Abraira C, Anderson RJ, et al. .; Control Group . Intensive glucose control and macrovascular outcomes in type 2 diabetes [published correction appears in Diabetologia 2009;52:2470] Diabetologia 2009;52:2288–2298 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
