

Parenchymal pericytes are not the major contributor of extracellular matrix in the fibrotic scar after stroke in male mice
- PMID: 31758600
- PMCID: PMC7154736
- DOI: 10.1002/jnr.24557
Parenchymal pericytes are not the major contributor of extracellular matrix in the fibrotic scar after stroke in male mice
Abstract
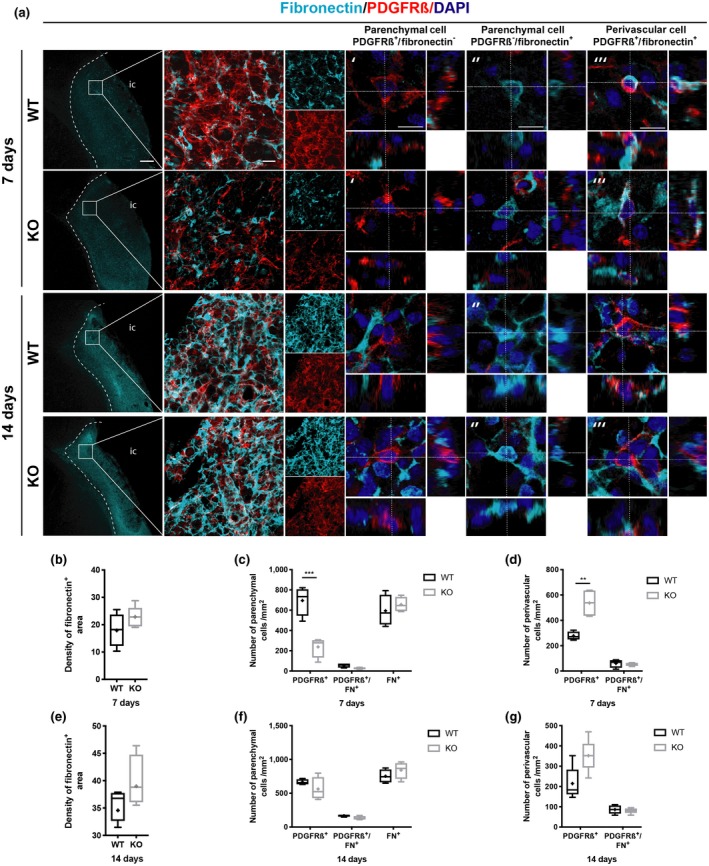
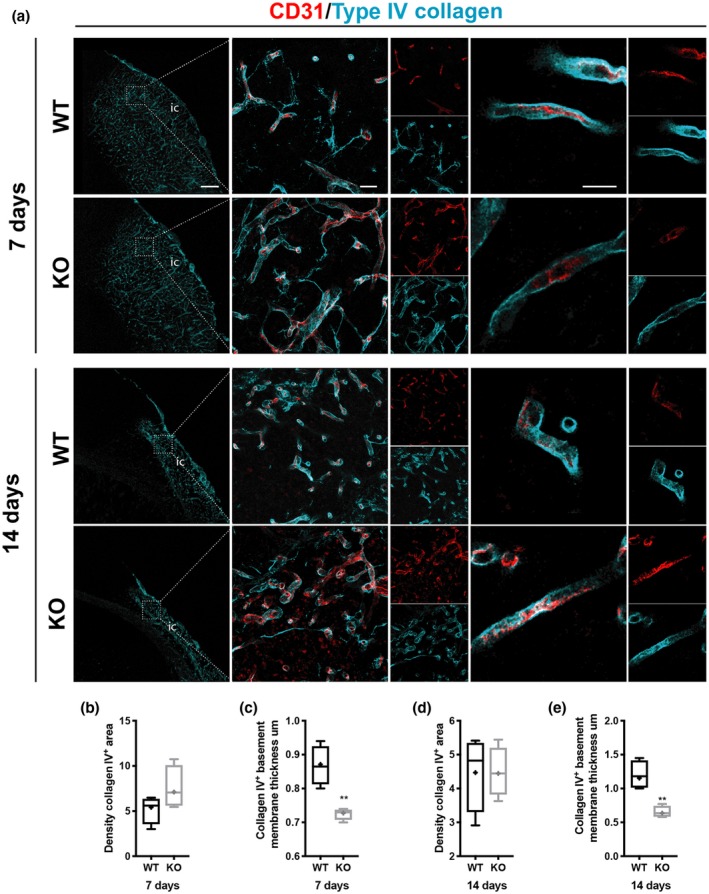
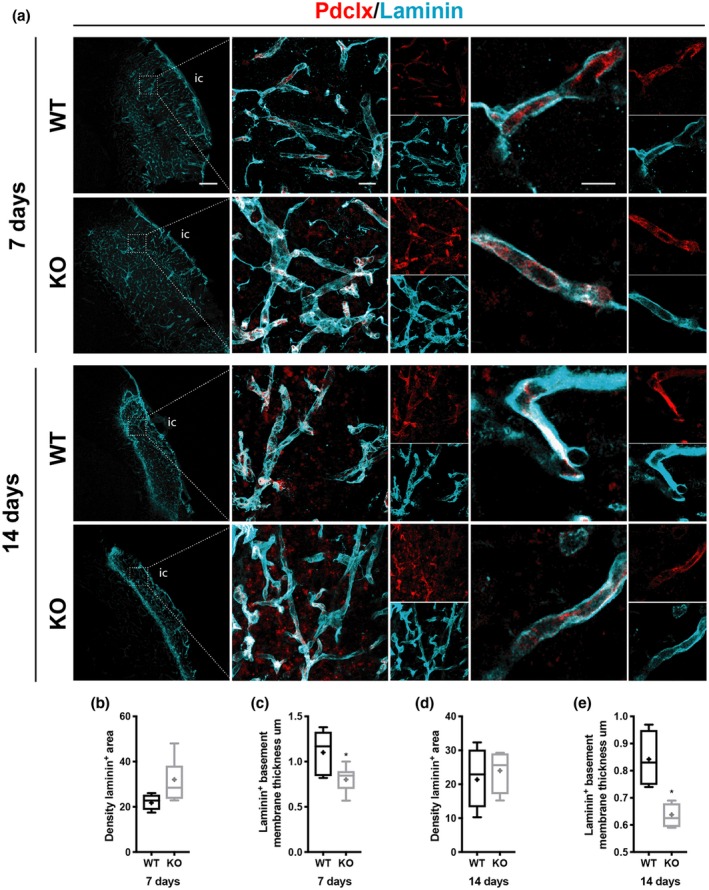
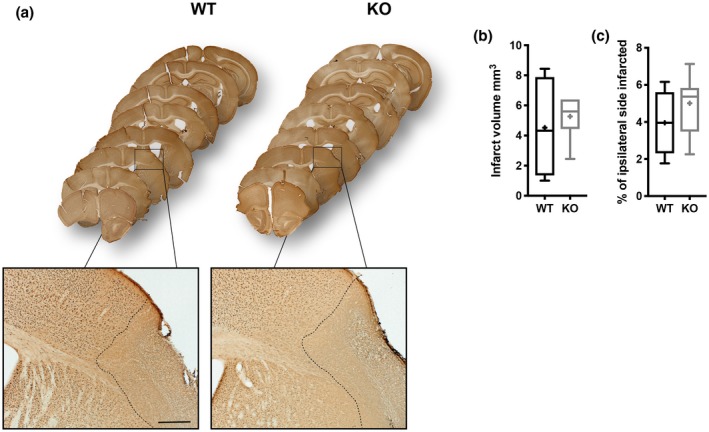
Scar formation after injury of the brain or spinal cord is a common event. While glial scar formation by astrocytes has been extensively studied, much less is known about the fibrotic scar, in particular after stroke. Platelet-derived growth factor receptor ß-expressing (PDGFRß+ ) pericytes have been suggested as a source of the fibrotic scar depositing fibrous extracellular matrix (ECM) proteins after detaching from the vessel wall. However, to what extent these parenchymal PDGFRß+ cells contribute to the fibrotic scar and whether targeting these cells affects fibrotic scar formation in stroke is still unclear. Here, we utilize male transgenic mice that after a permanent middle cerebral artery occlusion stroke model have a shift from a parenchymal to a perivascular location of PDGFRß+ cells due to the loss of regulator of G-protein signaling 5 in pericytes. We find that only a small fraction of parenchymal PDGFRß+ cells co-label with type I collagen and fibronectin. Consequently, a reduction in parenchymal PDGFRß+ cells by ca. 50% did not affect the overall type I collagen or fibronectin deposition after stroke. The redistribution of PDGFRß+ cells to a perivascular location, however, resulted in a reduced thickening of the vascular basement membrane and changed the temporal dynamics of glial scar maturation after stroke. We demonstrate that parenchymal PDGFRß+ cells are not the main contributor to the fibrotic ECM, and therefore targeting these cells might not impact on fibrotic scar formation after stroke.
Keywords: RRID:AB_2082660; RRID:AB_2105706; RRID:AB_2162497; RRID:AB_217595; RRID:AB_2298772; RRID:AB_298179; RRID:AB_305808; RRID:AB_354858; RRID:AB_393571; RRID:AB_467492; RRID:SCR_002798; RRID:SCR_003070; RRID:SCR_010279; collagen; extracellular matrix; fibronectin; fibrotic scar; glial scar; pericytes; stroke.
© 2019 The Authors. Journal of Neuroscience Research published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Bahrami, A. J. , Gunaje, J. J. , Hayes, B. J. , Riehle, K. J. , Kenerson, H. L. , Yeung, R. S. , … Mahoney, W. M., Jr . (2014). Regulator of G‐protein signaling‐5 is a marker of hepatic stellate cells and expression mediates response to liver injury. PLoS One, 9(10), e108505 10.1371/journal.pone.0108505 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
