

EUS-guided gastroenteric anastomosis as a bridge to definitive treatment in benign gastric outlet obstruction
- PMID: 31759034
- PMCID: PMC7039740
- DOI: 10.1016/j.gie.2019.11.017
EUS-guided gastroenteric anastomosis as a bridge to definitive treatment in benign gastric outlet obstruction
Abstract
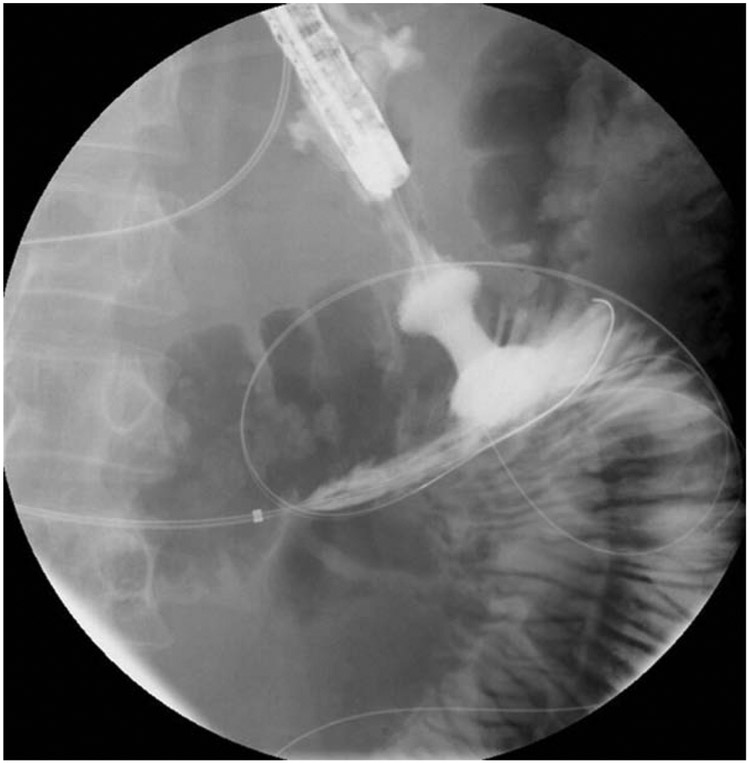
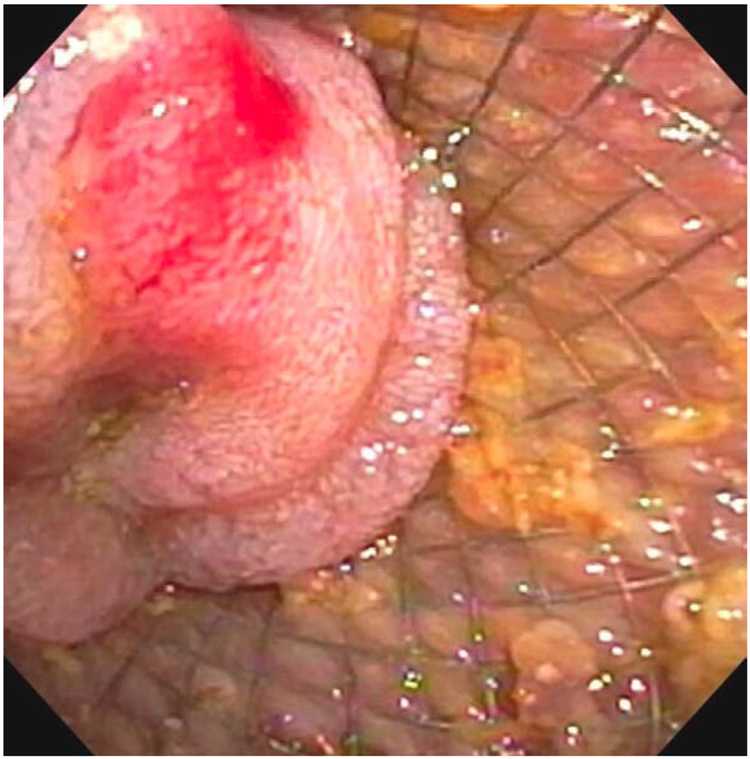
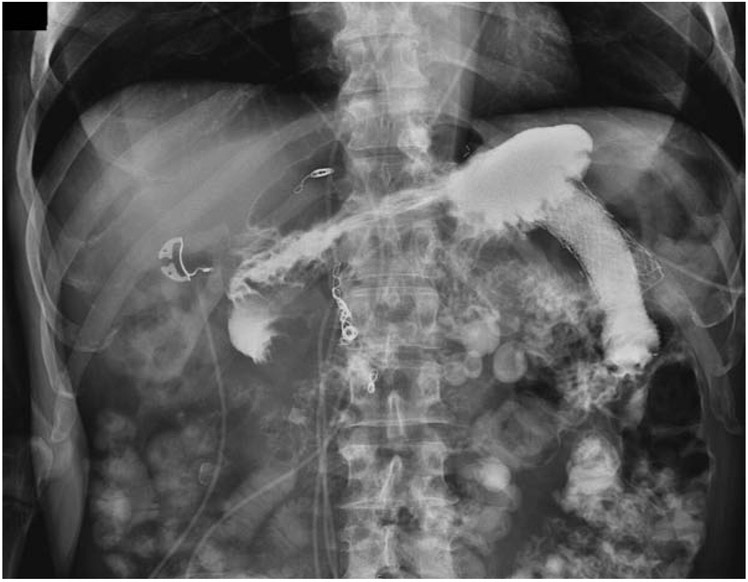
Background and aims: Benign gastric outlet obstruction (GOO) has typically been managed surgically. However, many patients are poor operative candidates because of comorbidities. EUS-guided gastroenterostomy (EUS-GE) using lumen-apposing metal stents (LAMSs) has previously demonstrated efficacy as a definitive treatment for benign and malignant GOO; however, limited data exist on use as a bridge to resolution of the obstruction in an attempt to avoid or delay definitive surgery.
Methods: A retrospective series of consecutive patients who underwent EUS-GE between January 2013 and July 2019 for benign GOO at a tertiary referral center were included in the study. The primary outcome was the rate of definitive surgery; secondary outcomes included technical success and rate of adverse events.
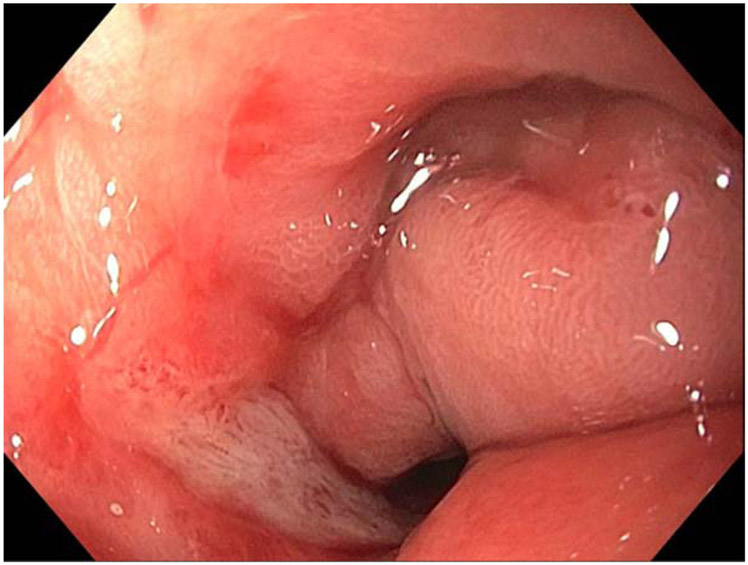
Results: During the study period, 22 patients with benign GOO underwent EUS-GE (40% female; mean age, 54.2 years). The mean procedure time was 66 minutes, and technical success was achieved in 21. Five patients developed recurrent GOO while the LAMS was in place after a mean dwell time of 228 days; 1 patient was converted to surgical GE. LAMSs were removed electively in 18 patients after GOO resolution and a mean dwell time of 270 days; 1 patient developed a recurrent GOO after LAMS removal and was converted to surgical GE. The rate of recurrent GOO after LAMS removal was 5.6%. Three severe adverse events occurred in the cohort.
Conclusions: EUS-GE was able to prevent surgery for GOO in 83.3% of cases. LAMSs needed to stay in place for a mean of 8.5 months to allow resolution of GOO, and there was a low rate of recurrent GOO (5.6%) after LAMS removal. Prospective, randomized trials comparing surgical and endoscopic anastomoses are needed in patients with benign causes of GOO.
Copyright © 2020 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Chowdhury A, Dhali GK, Banerjee PK. Etiology of gastric outlet obstruction. The American journal of gastroenterology. 1996. ;91:1679. - PubMed
-
- Johnson CD. Gastric outlet obstruction malignant until proved otherwise. The American journal of gastroenterology. 1995. ;90:1740. - PubMed
-
- Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. The American journal of gastroenterology. 2002. ;97:72. - PubMed
-
- Kochhar R, Malik S, Gupta P, Reddy YR, Dhaka N, Sinha SK, Gupta V, Noor MT, Mallick B. Etiological spectrum and response to endoscopic balloon dilation in patients with benign gastric outlet obstruction. Gastrointestinal endoscopy. 2018. ;88:899–908. - PubMed
-
- Rana SS. An overview of walled-off pancreatic necrosis for clinicians. Expert review of gastroenterology & hepatology. 2019. ;13:331–43. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
