

Recent Trends in Demographics, Surgery, and Prognosis of Patients with Surgically Resected Lung Cancer in a Single Institution from Korea
- PMID: 31760712
- PMCID: PMC6875437
- DOI: 10.3346/jkms.2019.34.e291
Recent Trends in Demographics, Surgery, and Prognosis of Patients with Surgically Resected Lung Cancer in a Single Institution from Korea
Abstract
Background: Over the past few decades, demographics information has changed significantly in patients with surgically resected lung cancer. Herein, we evaluated the recent trends in demographics, surgery, and prognosis of lung cancer surgery in Korea.
Methods: Patients with surgically resected primary lung cancer from 2002 to 2016 were retrospectively analyzed. Multivariable Cox regression analysis was conducted to identify prognostic factors for overall survival. The annual percent change (APC) and statistical significance were calculated using the Joinpoint software.
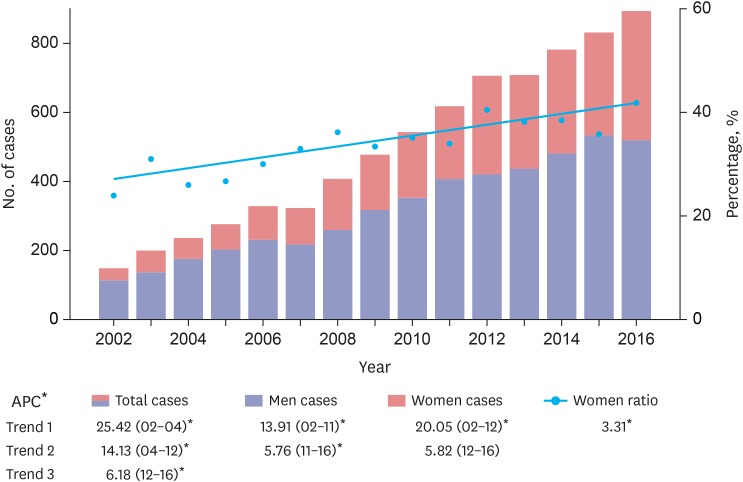
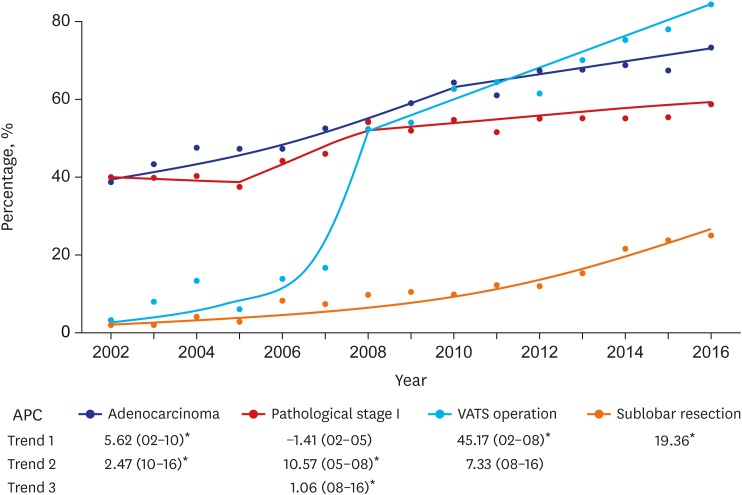
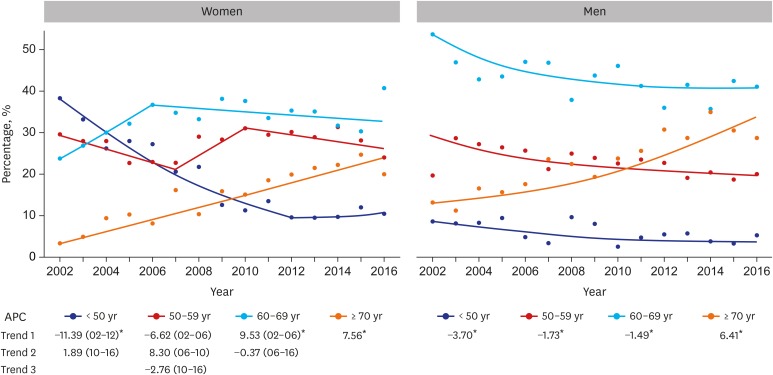
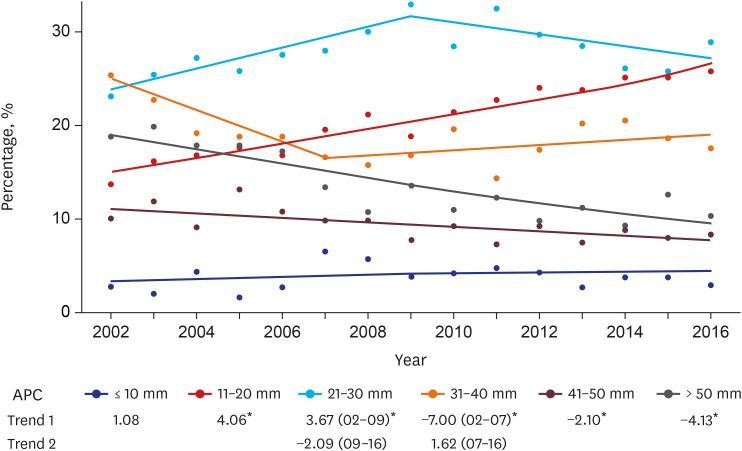
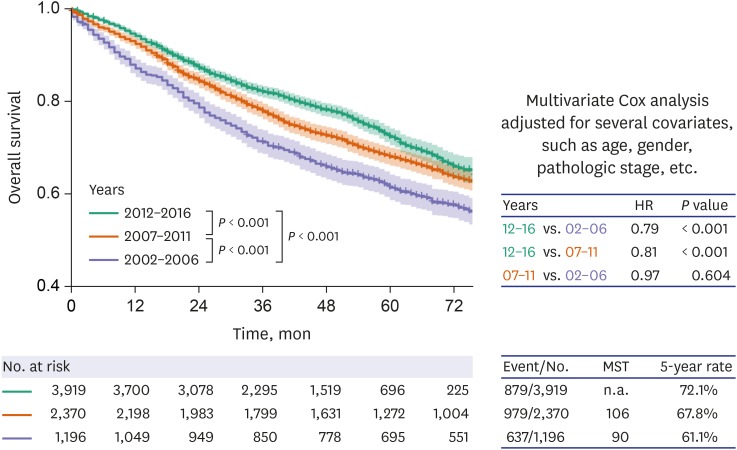
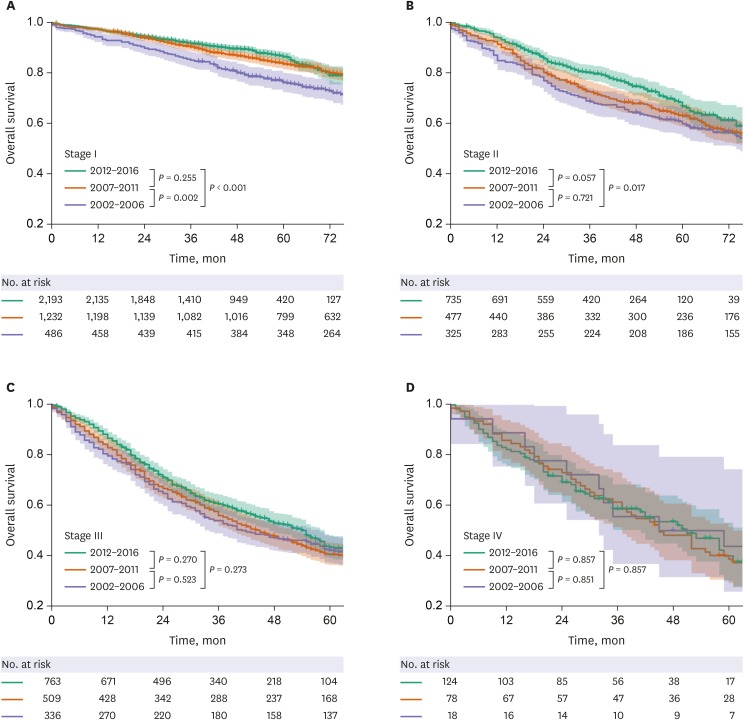
Results: A total of 7,495 patients were enrolled. Over the study period, the number of lung cancer surgeries continued to increase (P < 0.05). The proportion of women to total subjects has also increased (P < 0.05). The proportion of elderly patients (≥ 70 years) as well as those with tumors measuring 1-2 cm and 2-3 cm significantly increased in both genders (all P < 0.05). The proportion of patients with adenocarcinoma, video-assisted thoracic surgery, sublobar resection, and pathological stage I significantly increased (P < 0.05). The 5-year overall survival rate of lung cancer surgery increased from 61.1% in 2002-2006 to 72.1% in 2012-2016 (P < 0.001). The operative period was a significant prognostic factor in multivariable Cox analysis (P < 0.001).
Conclusion: The mean age of patients with lung cancer surgery increased gradually, whereas tumor size reduced. Prognosis of lung cancer surgery improved with recent increases in the frequency of adenocarcinoma, video-assisted thoracic surgery, sublobar resection, and pathological stage I. The operation period itself was also an independent prognostic factor for overall survival.
Keywords: Demography; Non-Small Cell Lung Cancer; Republic of Korea; Surgical Outcome; Surgical Resection; Time Trend.
© 2019 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Changes in the demographics and prognoses of patients with resected non-small cell lung cancer: a 20-year experience at a single institution in Korea.J Korean Med Sci. 2012 Dec;27(12):1486-90. doi: 10.3346/jkms.2012.27.12.1486. Epub 2012 Dec 7. J Korean Med Sci. 2012. PMID: 23255847 Free PMC article.
-
The prognostic role of pathologic invasive component size, excluding lepidic growth, in stage I lung adenocarcinoma.J Thorac Cardiovasc Surg. 2013 Sep;146(3):580-5. doi: 10.1016/j.jtcvs.2013.04.032. Epub 2013 Jun 15. J Thorac Cardiovasc Surg. 2013. PMID: 23778085
-
Current Trends of Lung Cancer Surgery and Demographic and Social Factors Related to Changes in the Trends of Lung Cancer Surgery: An Analysis of the National Database from 2010 to 2014.Cancer Res Treat. 2017 Apr;49(2):330-337. doi: 10.4143/crt.2016.196. Epub 2016 Jul 18. Cancer Res Treat. 2017. PMID: 27456943 Free PMC article.
-
Ten-Year Trends of Clinicopathologic Features and Surgical Treatment of Lung Cancer in China.Ann Thorac Surg. 2020 Feb;109(2):389-395. doi: 10.1016/j.athoracsur.2019.08.017. Epub 2019 Sep 14. Ann Thorac Surg. 2020. PMID: 31526778
-
[Survival after surgical treatment of bilateral synchronous multiple primary non-small cell lung cancers].Zhonghua Zhong Liu Za Zhi. 2016 Jun 23;38(6):460-5. doi: 10.3760/cma.j.issn.0253-3766.2016.06.011. Zhonghua Zhong Liu Za Zhi. 2016. PMID: 27346405 Chinese.
Cited by
-
JAK2 Loss Arising From Tumor-Spread-Through-Air-Spaces (STAS) Promotes Tumor Progression by Suppressing CD8+ T Cells in Lung Adenocarcinoma: A Machine Learning Approach.J Korean Med Sci. 2024 Jan 15;39(2):e16. doi: 10.3346/jkms.2024.39.e16. J Korean Med Sci. 2024. PMID: 38225784 Free PMC article.
-
Impact of microvascular invasion on 5-year overall survival of resected non-small cell lung cancer.J Bras Pneumol. 2022 Jul 8;48(3):e20210283. doi: 10.36416/1806-3756/e20210283. eCollection 2022. J Bras Pneumol. 2022. PMID: 35830051 Free PMC article.
-
Evaluation of Surgical Cases of Lung Cancer Admitted in Shiraz Referral Hospitals, Southern Iran in 2009-2022.Cancer Rep (Hoboken). 2025 Mar;8(3):e70108. doi: 10.1002/cnr2.70108. Cancer Rep (Hoboken). 2025. PMID: 40071520 Free PMC article.
-
Scorpiones, Scolopendra and Gekko Inhibit Lung Cancer Growth and Metastasis by Ameliorating Hypoxic Tumor Microenvironment via PI3K/AKT/mTOR/HIF-1α Signaling Pathway.Chin J Integr Med. 2024 Sep;30(9):799-808. doi: 10.1007/s11655-024-3803-8. Epub 2024 Jun 8. Chin J Integr Med. 2024. PMID: 38850481
-
Predicting Postoperative Complications and Long-Term Survival After Lung Cancer Surgery Using Eurolung Risk Score.J Korean Med Sci. 2022 Feb 7;37(5):e36. doi: 10.3346/jkms.2022.37.e36. J Korean Med Sci. 2022. PMID: 35132842 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e278S–e313S. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
