

Elevated HbA1c Is Associated with Altered Cortical and Trabecular Microarchitecture in Girls with Type 1 Diabetes
- PMID: 31761940
- PMCID: PMC7064304
- DOI: 10.1210/clinem/dgz221
Elevated HbA1c Is Associated with Altered Cortical and Trabecular Microarchitecture in Girls with Type 1 Diabetes
Abstract
Context: Skeletal fragility is a significant complication of type 1 diabetes (T1D), with an increased risk of fracture observed starting in childhood. Altered bone accrual and microarchitectural development during the critical peripubertal years may contribute to this fragility.
Objective: To evaluate differences in skeletal microarchitecture between girls with T1D and controls and to assess factors associated with these differences.
Design: Cross-sectional comparison.
Participants: Girls ages 10-16 years, 62 with T1D and 61 controls.
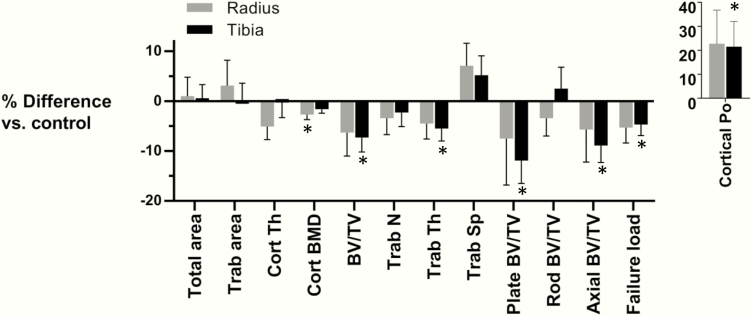
Results: Areal bone mineral density (BMD) measured by dual-energy x-ray absorptiometry did not differ between girls with and without T1D. At the distal tibia, trabecular BMD was 7.3 ± 2.9% lower in T1D (P = 0.013), with fewer plate-like and axially-aligned trabeculae. Cortical porosity was 21.5 ± 10.5% higher, while the estimated failure load was 4.7 ± 2.2% lower in T1D (P = 0.043 and P = 0.037, respectively). At the distal radius, BMD and microarchitecture showed similar differences between the groups but did not reach statistical significance. After stratifying by HbA1c, only those girls with T1D and HbA1c > 8.5% differed significantly from controls. P1NP, a marker of bone formation, was lower in T1D while CTX and TRAcP5b, markers of bone resorption and osteoclast number, respectively, did not differ. The insulin-like growth factor 1 (IGF-1) Z-score was lower in T1D, and after adjustment for the IGF-1 Z-score, associations between T1D status and trabecular microarchitecture were largely attenuated.
Conclusions: Skeletal microarchitecture is altered in T1D early in the course of disease and among those with higher average glycemia. Suppressed bone formation and lower circulating IGF-1 likely contribute to this phenotype.
Trial registration: ClinicalTrials.gov NCT02140424.
Keywords: bone density; microarchitecture; pediatrics; type 1 diabetes.
© Endocrine Society 2019. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures


References
-
- Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes--a meta-analysis. Osteoporos Int. Apr 2007;18(4):427–444. - PubMed
-
- Hygum K, Starup-Linde J, Harslof T, Vestergaard P, Langdahl BL.. MECHANISMS IN ENDOCRINOLOGY: Diabetes mellitus, a state of low bone turnover - a systematic review and meta-analysis. Eur J Endocrinol. Mar 2017;176(3):R137–R157. - PubMed
-
- Madsen JOB, Jorgensen NR, Pociot F, Johannesen J.. Bone turnover markers in children and adolescents with type 1 diabetes-A systematic review. Pediatr Diabetes. Aug 2019;20(5):510–522. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
