

Comparison of the Effects of Proximal Humeral Internal Locking System (PHILOS) Alone and PHILOS Combined with Fibular Allograft in the Treatment of Neer Three- or Four-part Proximal Humerus Fractures in the Elderly
- PMID: 31762222
- PMCID: PMC6904636
- DOI: 10.1111/os.12564
Comparison of the Effects of Proximal Humeral Internal Locking System (PHILOS) Alone and PHILOS Combined with Fibular Allograft in the Treatment of Neer Three- or Four-part Proximal Humerus Fractures in the Elderly
Abstract
Objective: To compare and analyze the clinical outcomes of the proximal humeral internal locking system (PHILOS) alone and the PHILOS combined with fibular allograft in the treatment of Neer three- and four-part proximal humerus fractures (PHF) in the elderly.
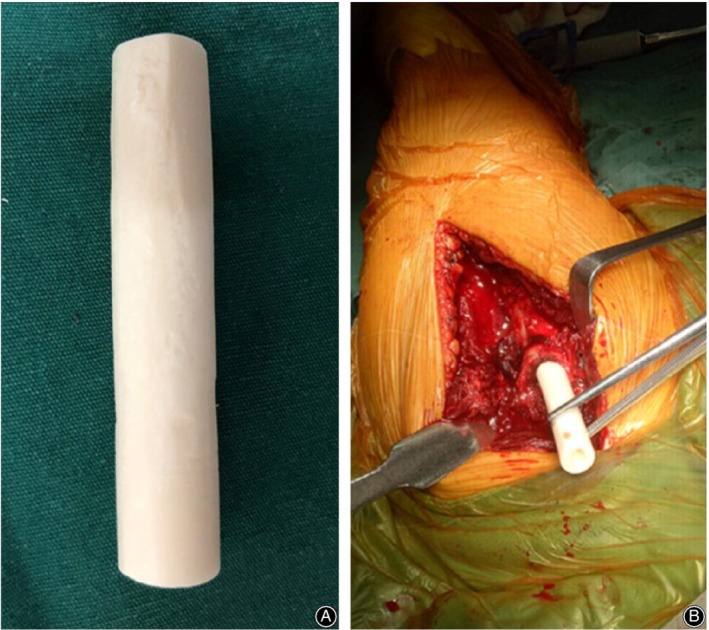
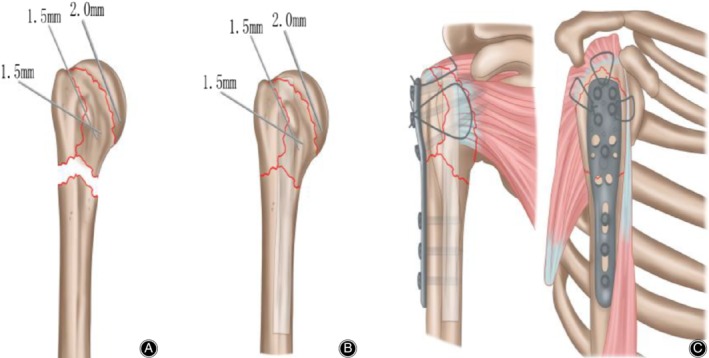
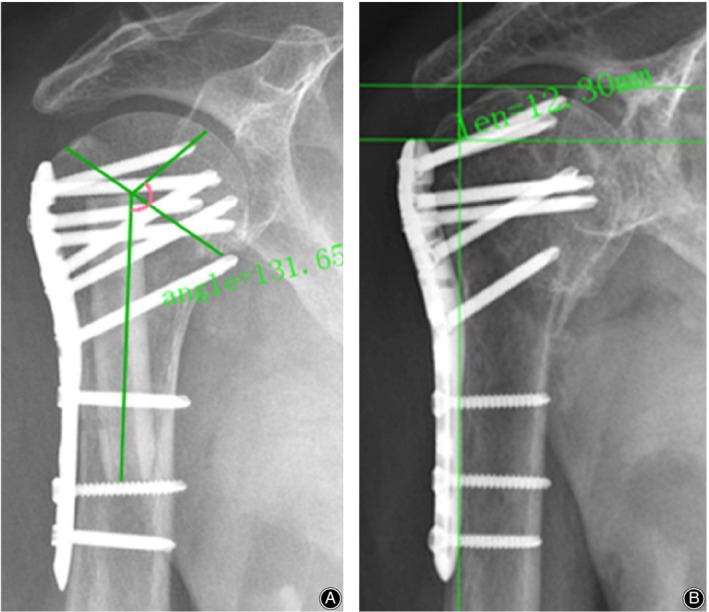
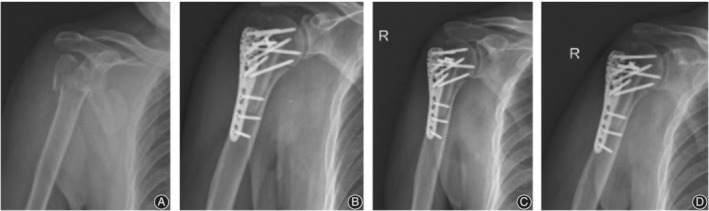
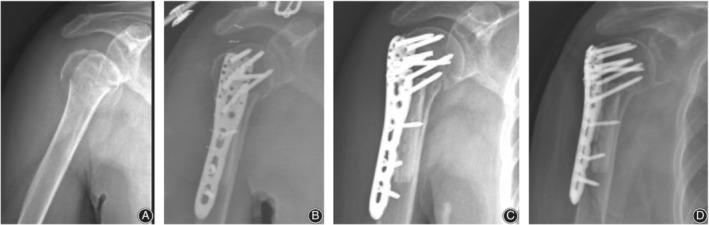
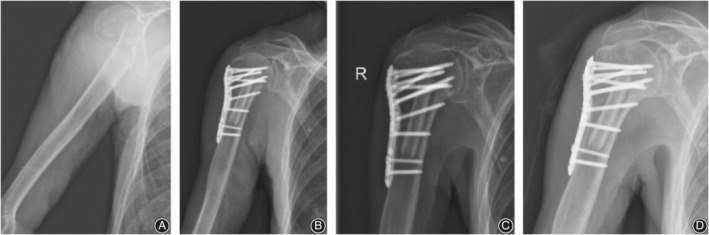
Methods: From January 2014 to January 2018, a total of 42 elderly patients with Neer three- or four-part PHF admitted to our hospital were randomly divided into observation group and control group, with 21 patients in each group. The observation group was treated with the PHILOS combined with fibular allograft. The control group was treated with the PHILOS alone. Perioperative parameters and fracture classification were recorded in the two groups. Function results were assessed by Visual Analog Scale (VAS), Constant-Murley score (CMS), American Shoulder and Elbow Surgeons (ASES) score, and the Disability of Arm-Shoulder-Hand (DASH) score. Radiological results were evaluated using the neck-shaft angle (NSA) and humeral head height (HHH), and complications were also recorded in each group.
Results: There were no significant differences between the two groups in terms of preoperative status, age, gender, cause of trauma, fracture site, and fracture classification. The average follow-up time was 12 months. At the last follow-up, the VAS and DASH observation groups were lower than the control group, and there was significant difference between the two groups (P < 0.05). The CMS and ASES were higher in the observation group than the control group, and there was significant difference between the two groups (P < 0.05). The mean difference in the NSA and HHH were lower in the observation group than the control group, and there was a significant difference between the two groups (P < 0.05). There was one postoperative complication in the observation group, which was humeral head avascular necrosis (AVN). There were seven postoperative complications in the control group, including three cases of humeral head collapse and three cases of screw cutout and one case of humeral head AVN. The incidence of postoperative complications in the observation group was significantly lower than the control group (P < 0.05), there was a significant difference between the two groups.
Conclusions: For Neer three- or four-part PHF in the elderly patients, PHILOS fixation with fibular allograft shows satisfactory short-term results with respect to humeral head support and maintenance of reduction, and may reduce the incidence of complications associated with fixation using a PHILOS alone.
Keywords: Anatomical allograft; Elderly; Fibular shaft; Proximal humeral internal locking system; Proximal humerus fractures.
© 2019 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures


References
-
- Wang MQ, Youssef T, Smerdely P. Incidence and outcomes of humeral fractures in the older person. Osteoporos Int, 2018, 29: 1601–1608. - PubMed
-
- Cai M, Tao K, Yang C, Li S. Internal fixation versus shoulder hemiarthroplasty for displaced 4‐part proximal humeral fractures in elderly patients. Orthopedics, 2012, 35: 748. - PubMed
-
- Chivot M, Lami D, Bizzozero P, Galland A, Argenson JN. Three‐ and four‐part displaced proximal humeral fractures in patients older than 70 years: reverse shoulder arthroplasty or nonsurgical treatment. J Shoulder Elbow Surg, 2019, 28: 252–259. - PubMed
-
- Lee SH, Han SS, Yoo BM, Kim JW. Outcomes of locking plate fixation with fibular allograft augmentation for proximal humeral fractures in osteoporotic patients. Bone Joint J., 2019, 101‐B: 260–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
