

Influence of Diabetic Distal Symmetric Polyneuropathy on the Performance of the Musculoskeletal System of Lower Leg and Foot
- PMID: 31762562
- PMCID: PMC6853727
- DOI: 10.5455/medarh.2019.73.262-267
Influence of Diabetic Distal Symmetric Polyneuropathy on the Performance of the Musculoskeletal System of Lower Leg and Foot
Abstract
Introduction: Complications on the lower extremities are a major cause of morbidity, disability, emotional and physical suffering in people with diabetes. Diabetic neuropathy (DN) is the most frequent complication of both types of diabetes. Lack of performance of the musculoskeletal system of lower leg and foot can results in high focal plantar pressures with increased ulceration risk in patients with neuropathy.
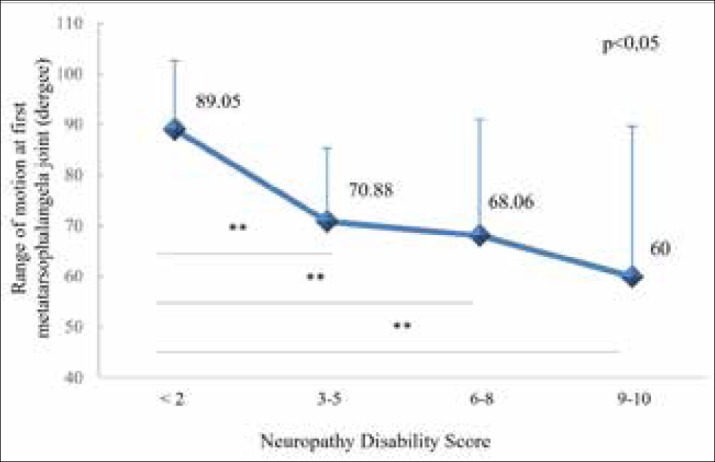
Aim: To determine the impact of the severity of distal symmetric polyneuropathy (DSPN) on the foot and ankle muscle strength and the range of motion (ROM) at ankle joint (AJ), subtalar joint (SJ) and first metatarsophalangeal joint (I MTP).
Methods: A cross-sectional study was conducted among 100 diabetic patients. The level of DSPN was assessed using the Neuropathy Disability Score. Function of ten foot and ankle muscles has been evaluated by manual muscle testing. Muscle strength was scored by semiquantitative grading system used in the Michigan Diabetic Neuropathy Score. ROM at the AJ, SJ and I MTP was measured with goniometer.
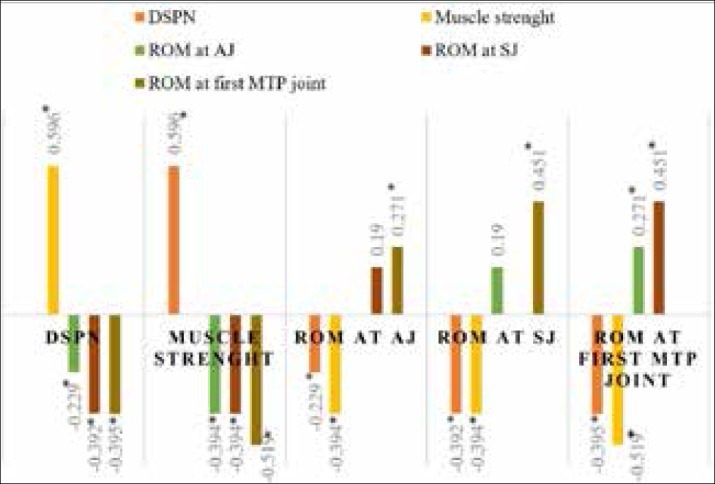
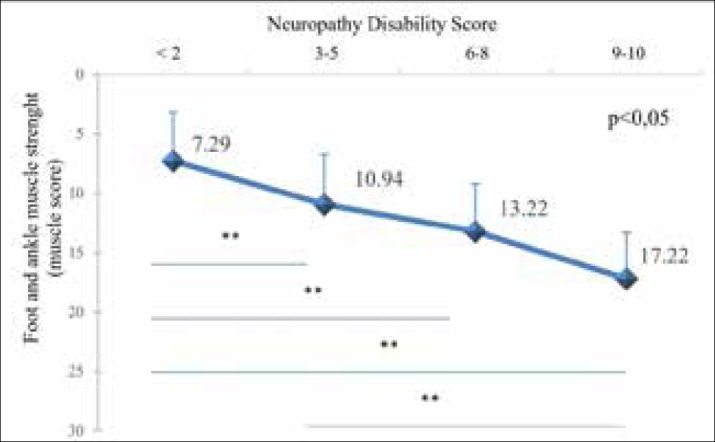
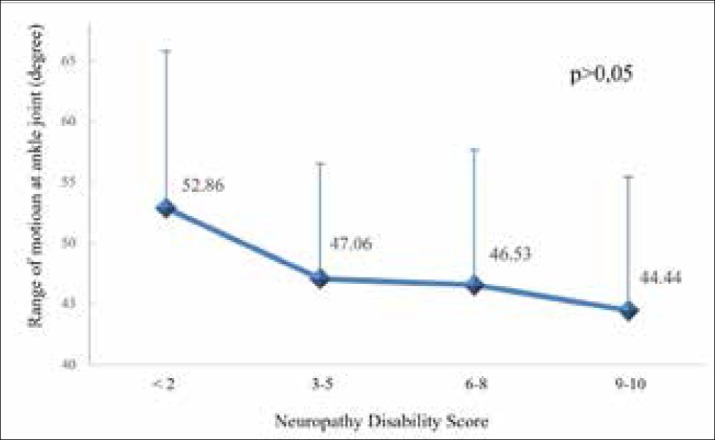
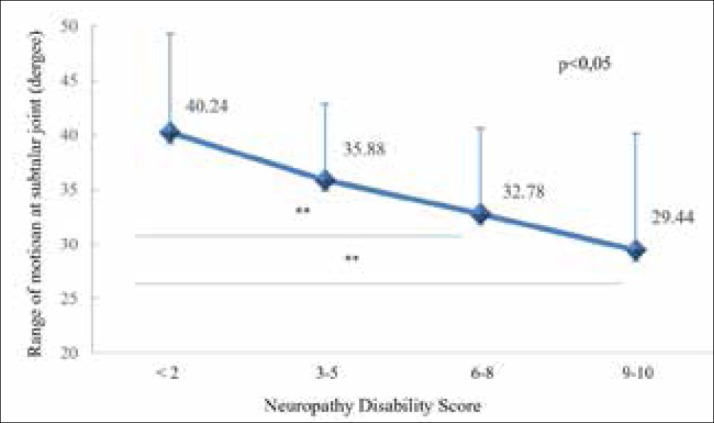
Results: The average patients age was 61.91±10.74 and diabetes duration 12.25±8.60 years. DSPN was present in 45% of patients. The average strength of foot and ankle muscles expressed by muscle score was 11.56±5.08. The average ROM at AJ was 47.85°, at SJ 35.10° and at I MTP 72.70°. Correlations between the severity of the DSPN and muscle function, ROM at AJ, SJ and I MTP were statistically significant. ROM at SJ and I MTP declines significantly with progression of neuropathy but not significant at AJ.
Conclusion: The severity of DSPN is significantly associated with foot and ankle muscle weakness and ROM at the SJ and the I MTP, but not significantly with the ROM at the AJ.
Keywords: Diabetes Mellitus; complications; muscles.
© 2019 Snjezana Novakovic Bursac, Slavica Jandric, Goran Talic.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
The relationship between passive range of motion and range of motion during gait and plantar pressure measurements.Diabet Med. 2007 Nov;24(11):1240-6. doi: 10.1111/j.1464-5491.2007.02233.x. Diabet Med. 2007. PMID: 17956451
-
Reduced Lower-Limb Muscle Strength and Volume in Patients With Type 2 Diabetes in Relation to Neuropathy, Intramuscular Fat, and Vitamin D Levels.Diabetes Care. 2016 Mar;39(3):441-7. doi: 10.2337/dc15-0995. Epub 2016 Jan 6. Diabetes Care. 2016. PMID: 26740641 Free PMC article.
-
The role of limited joint mobility in diabetic patients with an at-risk foot.Diabetes Care. 2004 Apr;27(4):942-6. doi: 10.2337/diacare.27.4.942. Diabetes Care. 2004. PMID: 15047653
-
Motor neuropathy.Handb Clin Neurol. 2014;126:81-95. doi: 10.1016/B978-0-444-53480-4.00007-2. Handb Clin Neurol. 2014. PMID: 25410216 Review.
-
Effect of three-week exercise program on muscle strength and joint mobility in patients with diabetic polyneuropathy: Randomized controlled trial.World J Diabetes. 2024 Dec 15;15(12):2311-2321. doi: 10.4239/wjd.v15.i12.2311. World J Diabetes. 2024. PMID: 39676803 Free PMC article. Review.
References
-
- International Diabetes Federation and International Working Group on the Diabetic Foot. Diabetes and Foot Care: Time to Act. Brussels (Belgium): International Diabetes Federation; 2005.
-
- International Diabetes Federation. Position Statement. Brussels, Belgium: International Diabetes Federation; 2015. The diabetic foot: amputations are preventable.
-
- American Diabetes Association. Preventive foot care in diabetes. Diabetes Care. 2004;27(1):63–64. - PubMed
-
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217–222. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical