

Pelvic congestion syndrome and embolization of pelvic varicose veins
- PMID: 31762775
- PMCID: PMC6852702
- DOI: 10.1590/1677-5449.190061
Pelvic congestion syndrome and embolization of pelvic varicose veins
Abstract
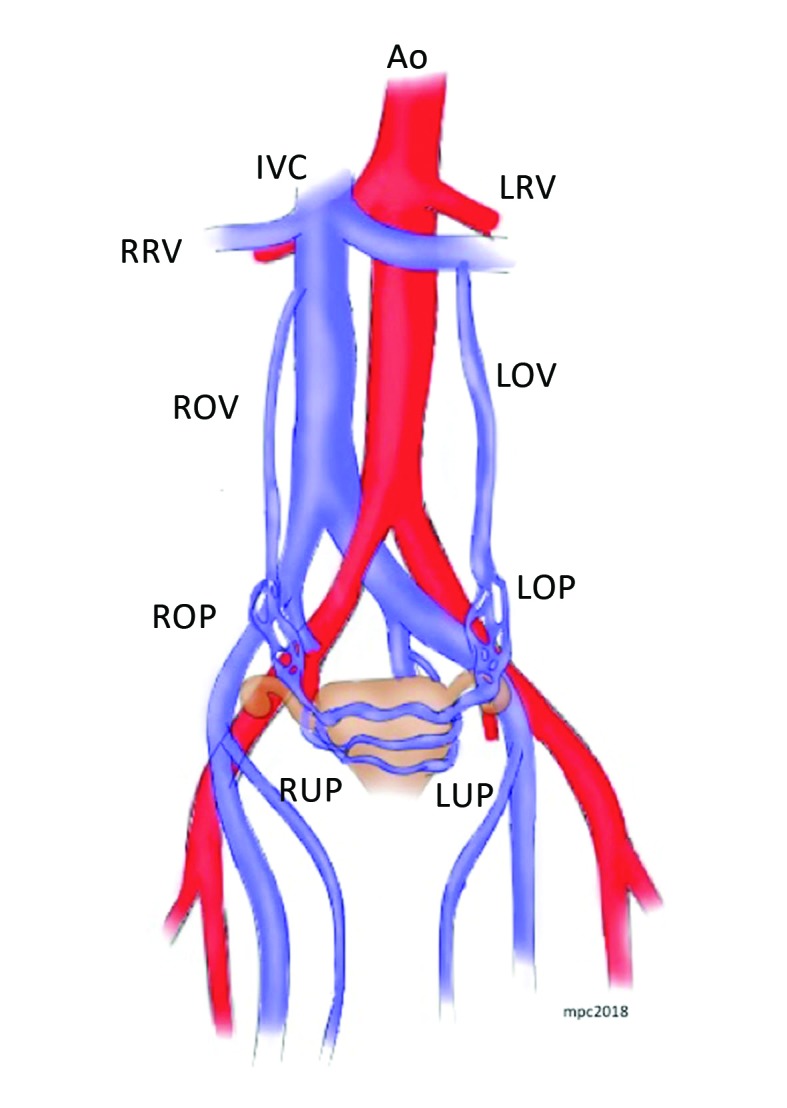
Pelvic congestion syndrome (PGS) is defined as chronic pelvic pain for more than 6 months associated with perineal and vulvar varicose veins caused by reflux or obstruction in gonadal, gluteal, or parauterine veins. PGS accounts for 16-31% of cases of chronic pelvic pain, and is usually diagnosed in the third and fourth decades of life. Interest in this condition among vascular surgeons has been increasing over recent years because of its association with venous insufficiency of the lower limbs. Despite its significant prevalence, PGS is still poorly diagnosed in both gynecology and angiology offices. Therefore, in this article we review the etiology and diagnosis of this condition and the outcomes of the different types of treatment available.
Resumo: A síndrome da congestão pélvica (SCP) é definida como dor pélvica crônica há mais de 6 meses associada a varizes perineais ou vulvares, resultantes do refluxo ou obstrução das veias gonadais, glúteas ou periuterinas. A SCP é responsável por 16-31% dos casos de dor pélvica crônica, sendo diagnosticada sobretudo na terceira e quarta décadas de vida. Nos últimos anos, houve um interesse maior nessa patologia por parte dos cirurgiões vasculares devido à sua associação com insuficiência venosa de membros inferiores. Apesar de prevalente, a SCP ainda é pouco diagnosticada tanto nos consultórios ginecológicos quanto nos de angiologistas. Portanto, neste artigo revisaremos a etiologia e o diagnóstico desta patologia e os resultados dos diversos tipos de tratamentos disponíveis.
Keywords: embolization; varicose veins; venous insufficiency.
Conflict of interest statement
Conflicts of interest: No conflicts of interest declared concerning the publication of this article.
Figures
References
-
- Lechter A, Lopez G, Martinez C, Camacho J. Anatomy of the gonadal veins: a reappraisal. Surgery. 1991;109(6):735–739. - PubMed
Publication types
LinkOut - more resources
Full Text Sources