

A pacemaker lead in the left ventricle: An "unexpected" finding?
- PMID: 31762840
- PMCID: PMC6859553
- DOI: 10.1016/j.jccase.2019.08.012
A pacemaker lead in the left ventricle: An "unexpected" finding?
Abstract
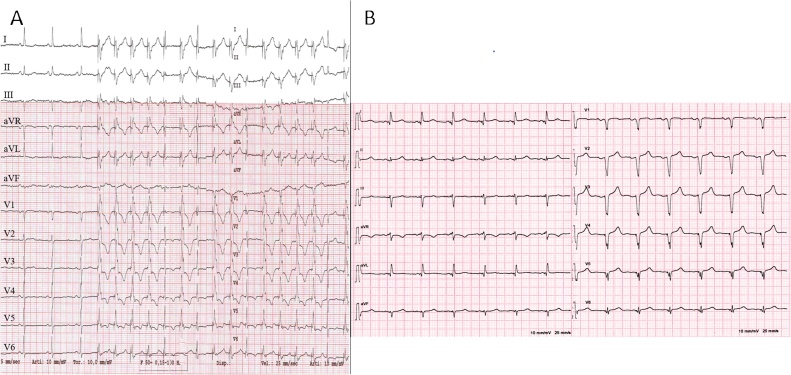
Inadvertent malposition of a pacemaker lead in the left ventricle is uncommon, but it should not be misdiagnosed. We report the case of a 68-year-old woman with symptomatic sick-sinus syndrome requiring pacemaker implantation. Shortly afterwards the lead was extracted and a new pacemaker was contralaterally implanted due to pocket hematoma and suspected lead fracture. Three months later, she was referred to our echocardiography laboratory complaining of asthenia. At transthoracic echocardiography an echo-bright linear structure was recognized in left atrium, passing through the mitral valve and leaning against the posterior left ventricular wall. In short-axis and apical views, the lead apparently crossed the interatrial septum through patent foramen ovale. The QRS-paced electrocardiogram showed right bundle branch block morphology. The lead was apparently well positioned, examining the chest X-ray postero-anterior view. On the contrary, by latero-lateral view and left-anterior oblique view, lead curvature was consistent with misplacement into the left ventricle. Malposition was confirmed by transesophageal echocardiography. Given the relatively recent implant, system revision with lead extraction was scheduled and completed without complications. This case report is intended to improve our awareness in the prevention and in the prompt detection of misplaced pacemaker leads in order to manage an immediate correction. <Learning objective: During lead implantation, fluoroscopic left-anterior oblique view should be always used to ensure correct positioning. At least 3-6 limb leads should be carefully monitored during the procedure, and a 12-lead standard electrocardiogram should be performed shortly afterwards for the paced QRS morphology. Lateral chest X-ray should always be taken after implantation. In cases of doubt, echocardiography (transthoracic or transesophageal) may confirm abnormal lead placement defining the route covered by the catheter.>.
Keywords: Echocardiography; Lead extraction; Lead malposition; Left ventricle; Pacemaker implantation.
© 2019 Published by Elsevier Ltd on behalf of Japanese College of Cardiology.
Figures


References
-
- Ohlow M.A., Roos M., Lauer B., Von Korn H., Geller J.C. Incidence, predictors, and outcome of inadvertent malposition of transvenous pacing or defibrillation lead in the left heart. Europace. 2016;18:1049–1054. - PubMed
-
- Ninot S., Sanchez G., Mestres C.A. An unusual travel of an endocardial pacing lead to the left ventricle. Interact Cardiovasc Thorac Surg. 2003;2:624–625. - PubMed
-
- van Gelder B.M., Bracke F.A., Oto A., Yildirir A., Haas P.C., Seger J.J. Diagnosis and management of inadvertently placed pacing and ICD leads in the left ventricle: a multicenter experience and review of the literature. Pacing Clin Electrophysiol. 2000;23:877–883. - PubMed
-
- Trohman R.G., Sharma P.S. Detecting and managing device leads inadvertently placed in the left ventricle. Cleve Clin J Med. 2018;85:69–75. - PubMed
-
- Klein H.O., Beker B., Sareli P., DiSegni E., Dean H., Kaplinsky E. Unusual QRS morphology associated with transvenous pacemakers. The pseudo RBBB pattern. Chest. 1985;87:517–521. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
