

Validation of the RayStation Monte Carlo dose calculation algorithm using a realistic lung phantom
- PMID: 31763759
- PMCID: PMC6909115
- DOI: 10.1002/acm2.12777
Validation of the RayStation Monte Carlo dose calculation algorithm using a realistic lung phantom
Abstract
Purpose: Our purposes are to compare the accuracy of RaySearch's analytical pencil beam (APB) and Monte Carlo (MC) algorithms for clinical proton therapy and to present clinical validation data using a novel animal tissue lung phantom.
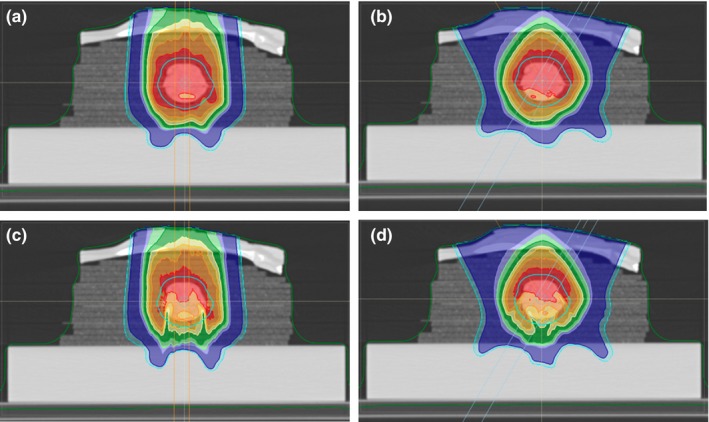
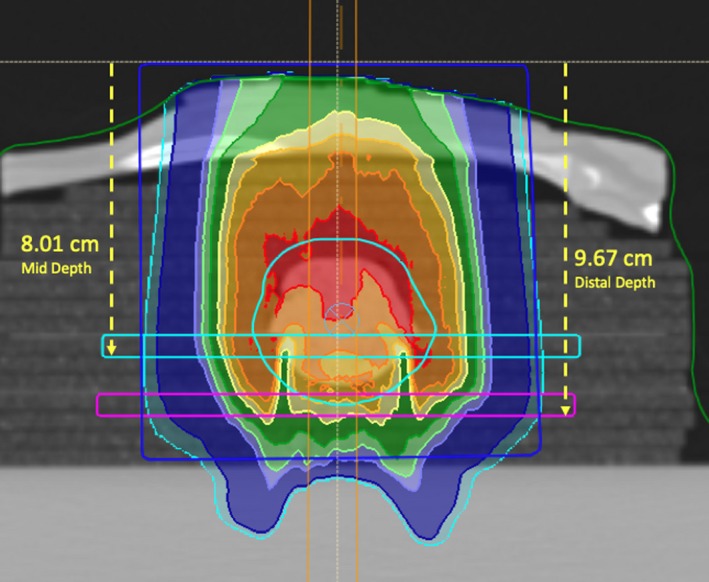
Methods: We constructed a realistic lung phantom composed of a rack of lamb resting on a stack of rectangular natural cork slabs simulating lung tissue. The tumor was simulated using 70% lean ground lamb meat inserted in a spherical hole with diameter 40 ± 5 mm carved into the cork slabs. A single-field plan using an anterior beam and a two-field plan using two anterior-oblique beams were delivered to the phantom. Ion chamber array measurements were taken medial and distal to the tumor. Measured doses were compared with calculated RayStation APB and MC calculated doses.
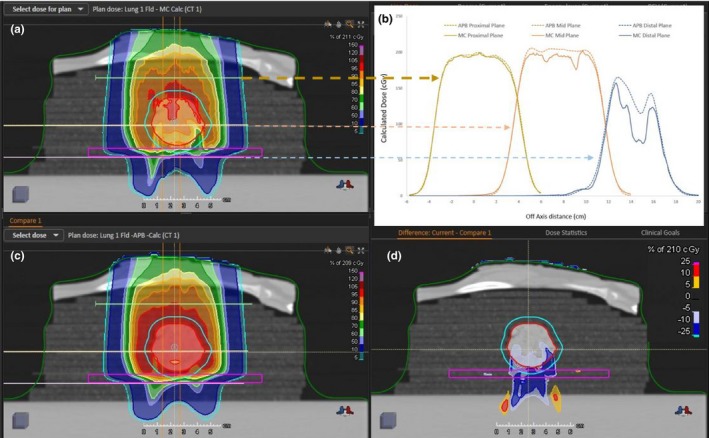
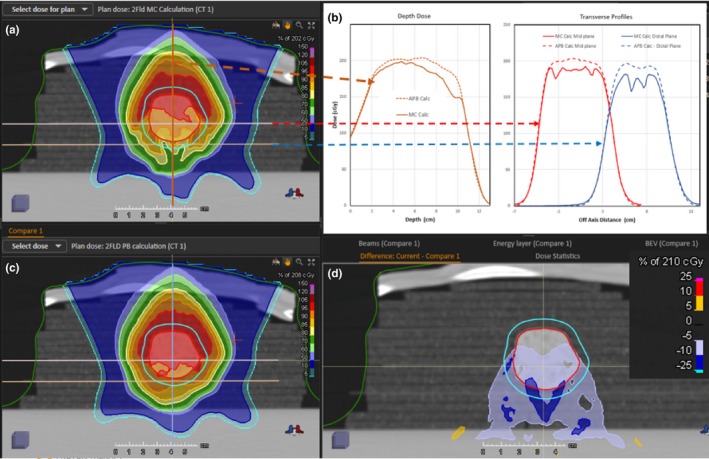
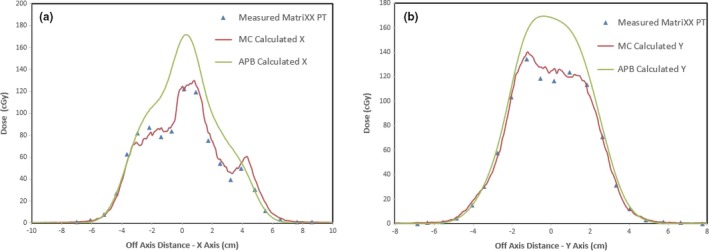
Results: Our lung phantom enabled measurements with the MatriXX PT at multiple depths in the phantom. Using the MC calculations, the 3%/3 mm gamma index pass rates, comparing measured with calculated doses, for the distal planes were 74.5% and 85.3% for the APB and 99.1% and 92% for the MC algorithms. The measured data revealed up to 46% and 30% underdosing within the distal regions of the target volume for the single and the two field plans when APB calculations are used. These discrepancies reduced to less than 18% and 7% respectively using the MC calculations.
Conclusions: RaySearch Laboratories' Monte Carlo dose calculation algorithm is superior to the pencil-beam algorithm for lung targets. Clinicians relying on the analytical pencil-beam algorithm should be aware of its pitfalls for this site and verify dose prior to delivery. We conclude that the RayStation MC algorithm is reliable and more accurate than the APB algorithm for lung targets and therefore should be used to plan proton therapy for patients with lung cancer.
Keywords: Monte Carlo; charged particle therapy; lung; pencil beam scanning; pencil-beam algorithm; radiation.
© 2019 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
No duality of interest disclosed.
Figures






References
-
- American Cancer Society . Cancer Facts & Figures 2018. Atlanta: American Cancer Society; 2018.
-
- Meinhold C, Abrahamson S, Adelstein S, et al. NCRP Report No. 116: Limitation of Exposure to Ionizing Radiation. Bethesda, MD: National Council on Radiation Protection and Measurements; 1993.
-
- Durante M, Paganetti H. Nuclear physics in particle therapy: a review. Rep Prog Phys. 2016;79:096702. - PubMed
-
- Nakamura N, Hotta K, Zenda S, et al. Hypofractionated proton beam therapy for centrally located lung cancer. Int J Radiat Oncol Biol Phys. 2018;102:e698. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
