

Central-Positive Complexes: A Novel Characterization of Ictal Markers Induced During Electroconvulsive Therapy
- PMID: 31764454
- PMCID: PMC6810820
- DOI: 10.1097/YCT.0000000000000597
Central-Positive Complexes: A Novel Characterization of Ictal Markers Induced During Electroconvulsive Therapy
Abstract
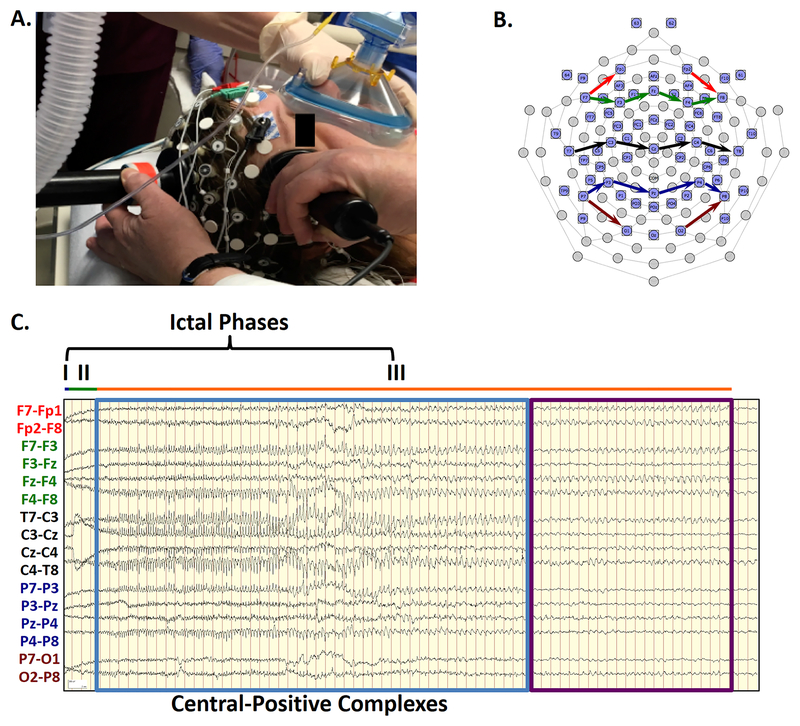
Objectives: Electroencephalography (EEG) allows monitoring of generalized seizures induced during electroconvulsive therapy (ECT). Scalp EEG recordings show different phases of electroencephalographic ictal activity during ECT seizures, documenting a pattern of seizures that may vary within and across individuals. In this case series, we used 64-electrode high-density EEG recording to detect topographic electroencephalographic changes not typically evident with conventional limited montages commonly used during ECT.
Methods: The EEG recordings were acquired from 5 participants (24 ECT sessions) during index courses for treatment-resistant depression. Using previously proposed staging criteria, the ictal EEG and simultaneously acquired video were interpreted by an expert reviewer blinded to study treatment parameters.
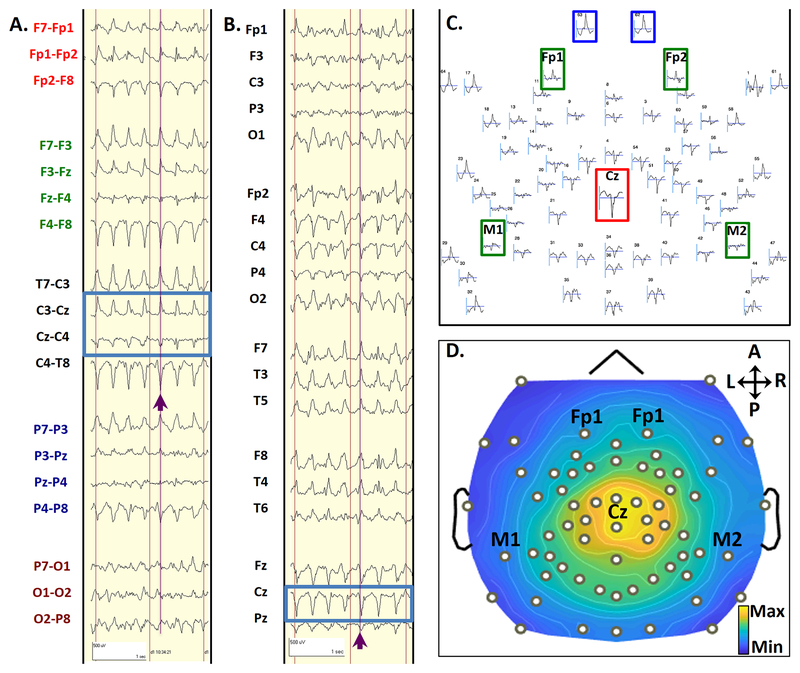
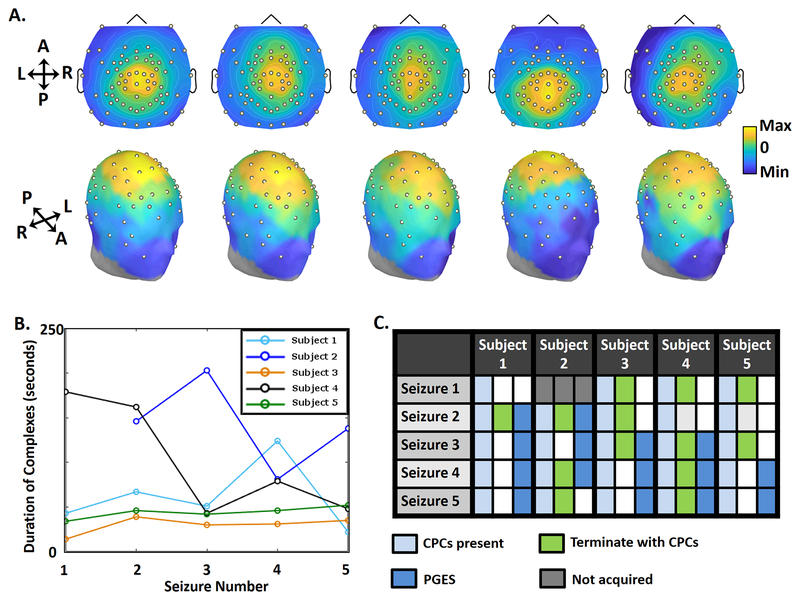
Results: The EEG recordings of all seizures showed generalized, high-amplitude, central-positive complexes (CPCs), which emerged at the beginning of phase III (polyspike and slow wave activity), with median duration of 47 seconds (interquartile range, 77 seconds), ranging from 14 to 203 seconds. Although individuals showed variability in frequency and amplitude of CPCs, CPCs typically evolved from 4.0 to 1.5 Hz in frequency and decreased in amplitude as the seizure progressed. Elaborating on previously described phases of ECT-induced electrographic seizures, we describe variability in morphology at seizure termination. Initiation of CPCs typically corresponded with clonic movements, but often terminated after motor signs ceased.
Conclusions: Generalized, high-amplitude, CPCs during ECT are a previously uncharacterized ictal waveform during ECT, which may have important scientific and clinical value. These complexes offer a specific marker for correlating clinical outcomes in ECT and greater understanding of generalized tonic-clonic seizures.
Conflict of interest statement
Conflicts of interest: The study was funded by the James S. McDonnell Foundation (US), Recipient: Michael S. Avidan, M.B.B.Ch. There are no other relevant conflicts of interest.
Figures
References
-
- Lisanby SH. Electroconvulsive therapy for depression. N Engl J Med 2007;357:1939–45. - PubMed
-
- Weiner RD. Indications for use of electroconvulsive therapy In: Weiner RD, ed. The Practice of Electroconvulsive Therapy: Recommendations for Treatment, Training, and Privileging (A Task Force Report of the American Psychiatric Association). Washington, D.C.: American Psychiatric Publishing, Inc.; 2000:5–26.
-
- Abrams R Electroconvulsive Therapy. 4th edition New York, NY: Oxford University Press; 2002.
-
- Krystal AD, Weiner RD. EEG correlates of the response to ECT: a possible antidepressant role of brain-derived neurotrophic factor. J ECT 1999;15:27–38. - PubMed
-
- Mayur P. Ictal electroencephalographic characteristics during electroconvulsive therapy: a review of determination and clinical relevance. J ECT 2006;22:213–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
