

Clinical review on triglycerides
- PMID: 31764986
- PMCID: PMC6938588
- DOI: 10.1093/eurheartj/ehz785
Clinical review on triglycerides
Abstract
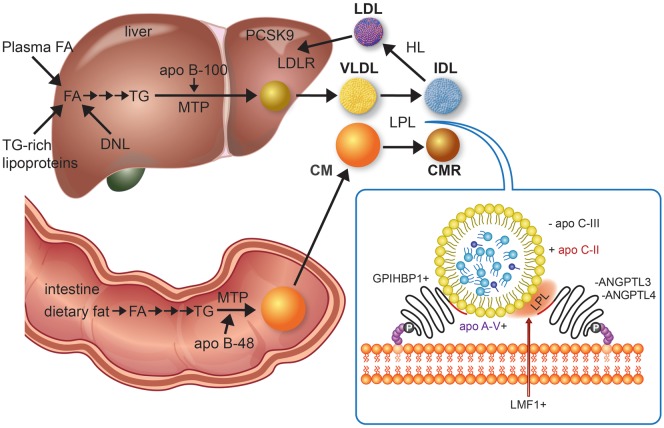
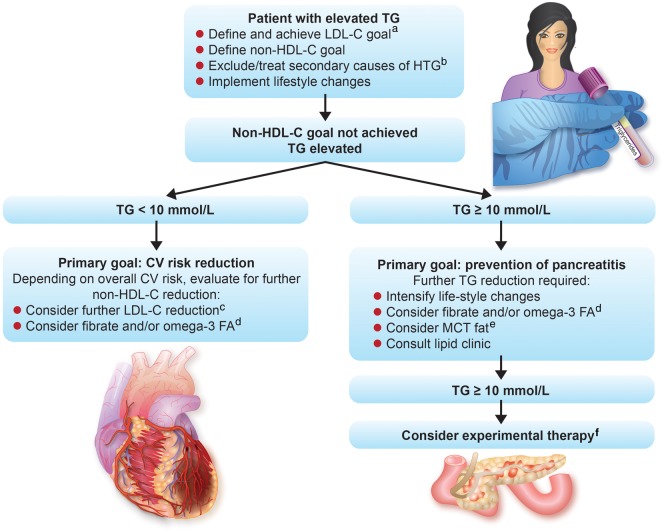
Hypertriglyceridaemia is a common clinical problem. Epidemiologic and genetic studies have established that triglyceride-rich lipoproteins (TRL) and their remnants as important contributors to ASCVD while severe hypertriglyceridaemia raises risk of pancreatitis. While low-density lipoprotein is the primary treatment target for lipid lowering therapy, secondary targets that reflect the contribution of TRL such as apoB and non-HDL-C are recommended in the current guidelines. Reduction of severely elevated triglycerides is important to avert or reduce the risk of pancreatitis. Here we discuss interventions for hypertriglyceridaemia, including diet and lifestyle, established treatments such as fibrates and omega-3 fatty acid preparations and emerging therapies, including various biological agents.
Keywords: Hypertriglyceridaemia; Lipoproteins; Review; Treatment; Triglycerides.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Dron JS, Wang J, Cao H, McIntyre AD, Iacocca MA, Menard JR, Movsesyan I, Malloy MJ, Pullinger CR, Kane JP, Hegele RA.. Severe hypertriglyceridemia is primarily polygenic. J Clin Lipidol 2019;13:80–88. - PubMed
-
- Hegele RA, Ginsberg HN, Chapman MJ, Nordestgaard BG, Kuivenhoven JA, Averna M, Borén J, Bruckert E, Catapano AL, Descamps OS, Hovingh GK, Humphries SE, Kovanen PT, Masana L, Pajukanta P, Parhofer KG, Raal FJ, Ray KK, Santos RD, Stalenhoef AFH, Stroes E, Taskinen M-R, Tybjærg-Hansen A, Watts GF, Wiklund O; European Atherosclerosis Society Consensus Panel. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol 2014;2:655–666. - PMC - PubMed
-
- Jaross W, Assmann G, Bergmann S, Schulte H.. Comparison of risk factors for coronary heart disease in Dresden and Munster. Results of the DRECAN (Dresden Cardiovascular Risk and Nutrition) study and the PROCAM (Prospective Cardiovascular Munster) Study. Eur J Epidemiol 1994;10:307–315. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
