

Longitudinal Investigation of Older Adults' Ability to Self-Manage Complex Drug Regimens
- PMID: 31765007
- PMCID: PMC7056504
- DOI: 10.1111/jgs.16255
Longitudinal Investigation of Older Adults' Ability to Self-Manage Complex Drug Regimens
Abstract
Objectives: We sought to investigate older patients' ability to correctly and efficiently dose multidrug regimens over nearly a decade and to explore factors predicting declines in medication self-management.
Design: Longitudinal cohort study funded by the National Institute on Aging.
Setting: One academic internal medicine clinic and six community health centers.
Participants: Beginning in 2008, 900 English-speaking adults, aged 55 to 74 years, were enrolled in the study, completing a baseline (T1) assessment. To date, 303 participants have completed the same assessment 9 years postbaseline (T4).
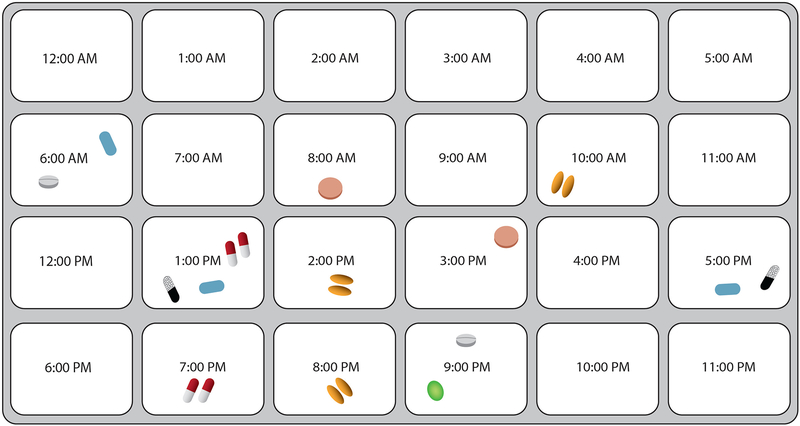
Measurements: At T1, subjects were given a standardized, seven-drug regimen and asked to demonstrate how they would take medicine over 24 hours. The number of dosing errors made and times per day that a participant would take medicine were recorded. Health literacy was measured via the Newest Vital Sign, and cognitive decline was measured by the Mini-Mental State Examination.
Results: Participants on average made 2.9 dosing errors (SD = 2.5 dosing errors; range = 0-21 dosing errors) of 21 potential errors at T1 and 5.0 errors (SD = 2.1 errors; range = 1-18 errors; P < .001) at T4. In a multivariate model, limited literacy (β = .69; 95% confidence interval [CI] = .18-1.20; P = .01), meaningful cognitive decline (β = 1.72; 95% CI = .70-2.74; P = .01), number of chronic conditions (β = .21; 95% CI = .07-.34; P = .01), and number of baseline dosing errors (β = -.76; 95% CI = -.85 to -.67; P < .001) were significant, independent predictors of changes in dosing errors. Most patients overcomplicated their daily medication schedule; no sociodemographic characteristics were predictive of poor regimen organization in multivariate models. In a multivariate model, there were no significant predictors of changes in regimen consolidation over time, except regimen consolidation at T1.
Conclusions: Older patients frequently overcomplicated drug regimens and increasingly made more dosing errors over 9 years of follow-up. Patients with limited literacy, cognitive decline, and multimorbidity were at greatest risk for errors. J Am Geriatr Soc 68:569-575, 2020.
Keywords: health literacy; medication safety; polypharmacy.
© 2019 The American Geriatrics Society.
Conflict of interest statement
Conflict of Interest
Stacy Bailey has served as a consultant to Merck, Sharp & Dohme Corp, Northwestern University/Gordon and Betty Moore Foundation, Pfizer, Inc and Luto LLC for work unrelated to this manuscript. She has also received funding support via her institution from Merck, Sharp & Dohme Corp and Eli Lilly and Company. Michael Wolf has served as a consultant to Merck, Sharp & Dohme Corp, Abbvie, Vivus, Inc., Luto LLC, Pfizer, Inc, Anheuser Busch Imbev, DenverHealth, and Teva Pharmaceuticals for work unrelated to this manuscript. He also has received funding support via his institution from Merck, Sharp & Dohme Corp, Eli Lilly and Company, Abbvie, and UnitedHealthcare. Other authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript.
Figures
References
-
- National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-term Trends in Health. Hyattsville, MD; 2017. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
