

Heterogeneity and efficacy of antipsychotic treatment for schizophrenia with or without treatment resistance: a meta-analysis
- PMID: 31766049
- PMCID: PMC7021799
- DOI: 10.1038/s41386-019-0577-3
Heterogeneity and efficacy of antipsychotic treatment for schizophrenia with or without treatment resistance: a meta-analysis
Abstract
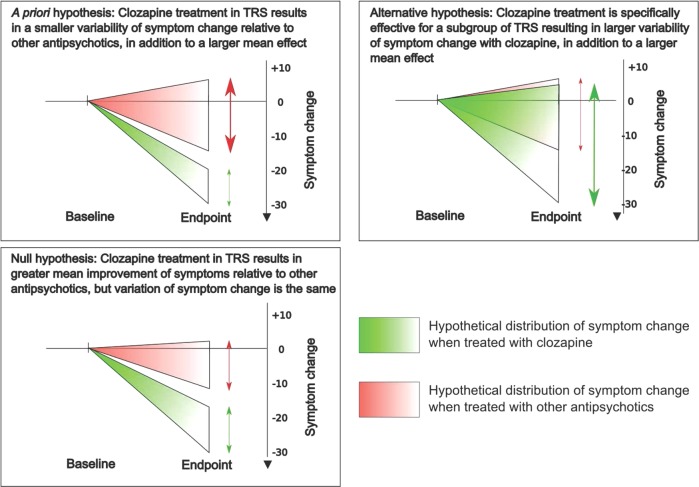
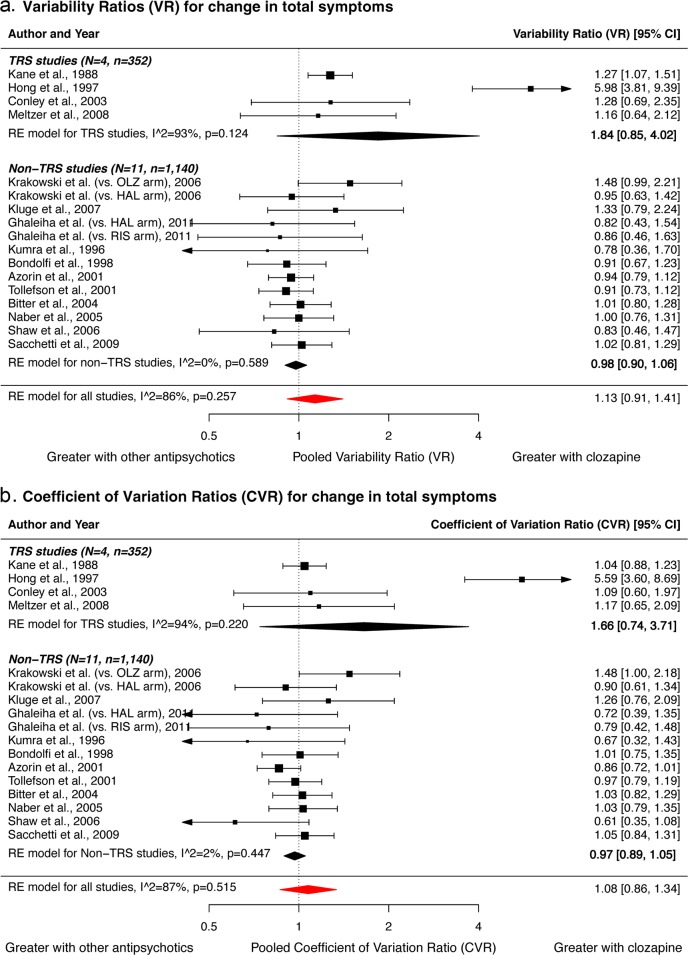
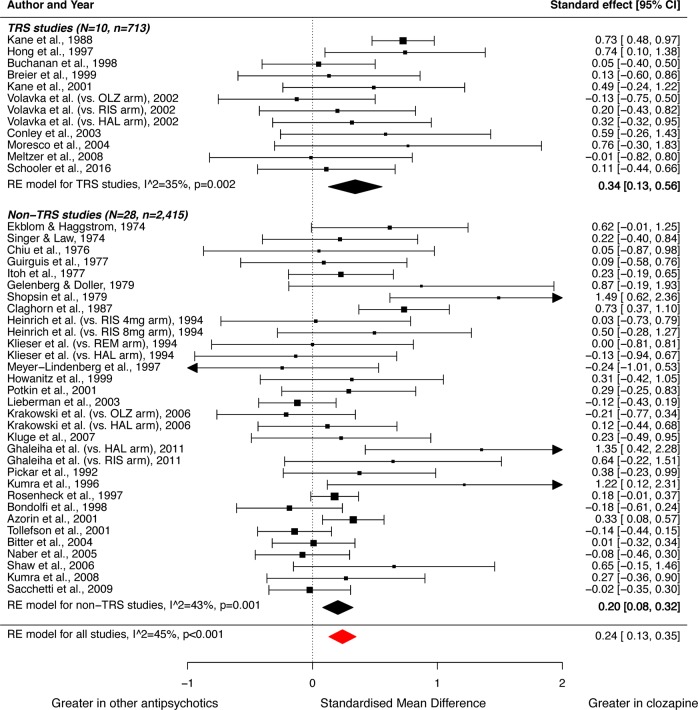
Two important clinical questions are whether there is a subtype of schizophrenia which responds differently to clozapine relative to other antipsychotics, and whether greater efficacy of clozapine is dependent on the degree of treatment-resistance. The authors address this by examining both variability and magnitude of response in patients treated with clozapine and other antipsychotics for both treatment-resistant schizophrenia (TRS) and non-resistant schizophrenia. Double-blind randomised controlled trials comparing clozapine with other antipsychotics in patients with schizophrenia were identified using five databases. Standard deviations and means of change in total, positive, and negative symptoms were extracted. Variability ratio (VR) and coefficient of variation ratio (CVR) were used to quantify relative variability in symptom change. Hedges' g was used to quantify mean differences. Ten TRS studies (n = 822) and 29 non-TRS studies (n = 2566) were meta-analysed. Relative variability in change of total symptoms did not differ significantly between clozapine and other antipsychotics in TRS studies (VR = 1.84; 95%CI, 0.85-4.02). These findings were similar with CVR, and for positive and negative symptoms. Clozapine was superior to other antipsychotics in improving total symptoms in both TRS (g = 0.34; 95%CI, 0.13-0.56) and non-TRS (g = 0.20; 95%CI, 0.08-0.32) studies. Furthermore, clozapine was superior in improving positive symptoms in both study groups, but not for negative symptoms. Pooled effect sizes showed no significant difference between TRS and non-TRS studies. These findings do not support a subtype of schizophrenia which responds specifically to clozapine. Clozapine is more effective than other antipsychotics irrespective of treatment-resistance, arguing for its use more generally in schizophrenia. PROSPERO CRD42018086507.
Figures
References
-
- Agid O, Arenovich T, Sajeev G, Zipursky RB, Kapur S, Foussias G, et al. An algorithm-based approach to first-episode schizophrenia: response rates over 3 prospective antipsychotic trials with a retrospective data analysis. J Clin Psychiatry. 2011;72:1439–44. doi: 10.4088/JCP.09m05785yel. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
