

Hospital Malnutrition, a Call for Political Action: A Public Health and NutritionDay Perspective
- PMID: 31766583
- PMCID: PMC6947230
- DOI: 10.3390/jcm8122048
Hospital Malnutrition, a Call for Political Action: A Public Health and NutritionDay Perspective
Abstract
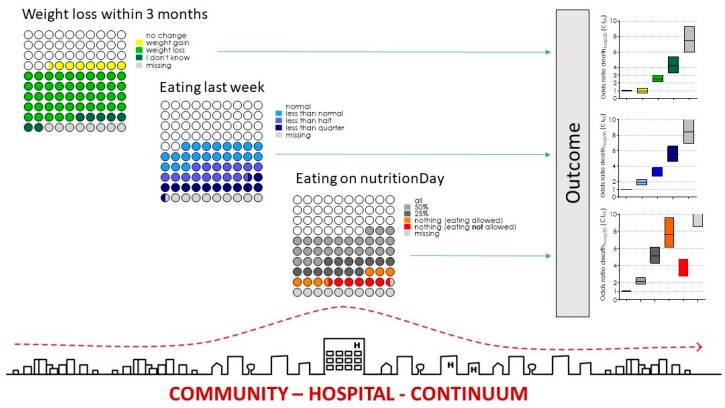
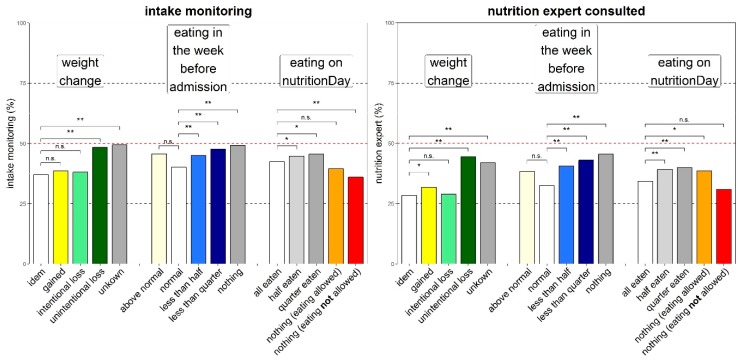
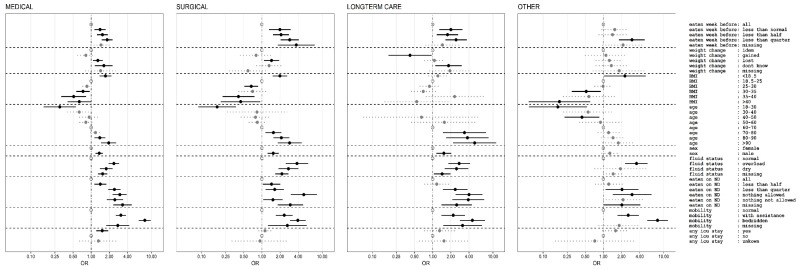
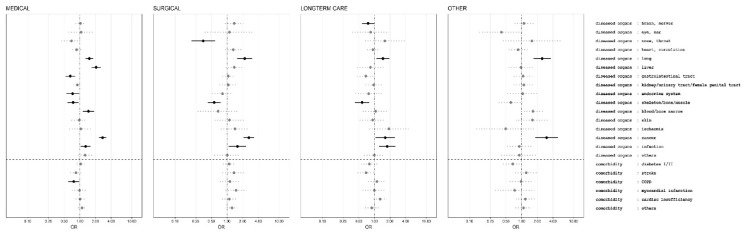
Disease-related malnutrition (DRM) is prevalent in hospitals and is associated with increased care needs, prolonged hospital stay, delayed rehabilitation and death. Nutrition care process related activities such as screening, assessment and treatment has been advocated by scientific societies and patient organizations but implementation is variable. We analysed the cross-sectional nutritionDay database for prevalence of nutrition risk factors, care processes and outcome for medical, surgical, long-term care and other patients (n = 153,470). In 59,126 medical patients included between 2006 and 2015 the prevalence of recent weight loss (45%), history of decreased eating (48%) and low actual eating (53%) was more prevalent than low BMI (8%). Each of these risk factors was associated with a large increase in 30 days hospital mortality. A similar pattern is found in all four patient groups. Nutrition care processes increase slightly with the presence of risk factors but are never done in more than 50% of the patients. Only a third of patients not eating in hospital receive oral nutritional supplements or artificial nutrition. We suggest that political action should be taken to raise awareness and formal education on all aspects related to DRM for all stakeholders, to create and support responsibilities within hospitals, and to create adequate reimbursement schemes. Collection of routine and benchmarking data is crucial to tackle DRM.
Keywords: benchmarking; continuity of care; disease related malnutrition.; hospital; malnutrition; mortality; nutrition care; process indicators.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Council of Europe Committee of Ministers Resolution ResAP (2003) 3 on Food and Nutritional Care in Hospitals. [(accessed on 18 November 2019)]; Available online: https://search.coe.int/
-
- Hiesmayr M., Schindler K., Pernicka E., Schuh C., Schoeniger-Hekele A., Bauer P., Laviano A., Lovell A.D., Mouhieddine M., Schuetz T., et al. Decreased food intake is a risk factor for mortality in hospitalised patients: The NutritionDay survey 2006. Clin. Nutr. 2009;28:484–491. doi: 10.1016/j.clnu.2009.05.013. - DOI - PubMed
-
- Hiesmayr M., Frantal S., Schindler K., Themessl-Huber M., Mouhieddine M., Schuh C., Pernicka E., Schneider S., Singer P., Ljunqvist O., et al. The Patient- And Nutrition-Derived Outcome Risk Assessment Score (PANDORA): Development of a Simple Predictive Risk Score for 30-Day In-Hospital Mortality Based on Demographics, Clinical Observation, and Nutrition. PLoS ONE. 2015;10:e0127316. doi: 10.1371/journal.pone.0127316. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
