

Fertility-sparing trachelectomy for early-stage cervical cancer: A proposal of an ideal candidate
- PMID: 31767188
- PMCID: PMC7526083
- DOI: 10.1016/j.ygyno.2019.11.021
Fertility-sparing trachelectomy for early-stage cervical cancer: A proposal of an ideal candidate
Abstract
Objective: To propose an ideal patient candidate with early-stage cervical cancer for undergoing fertility-sparing trachelectomy.
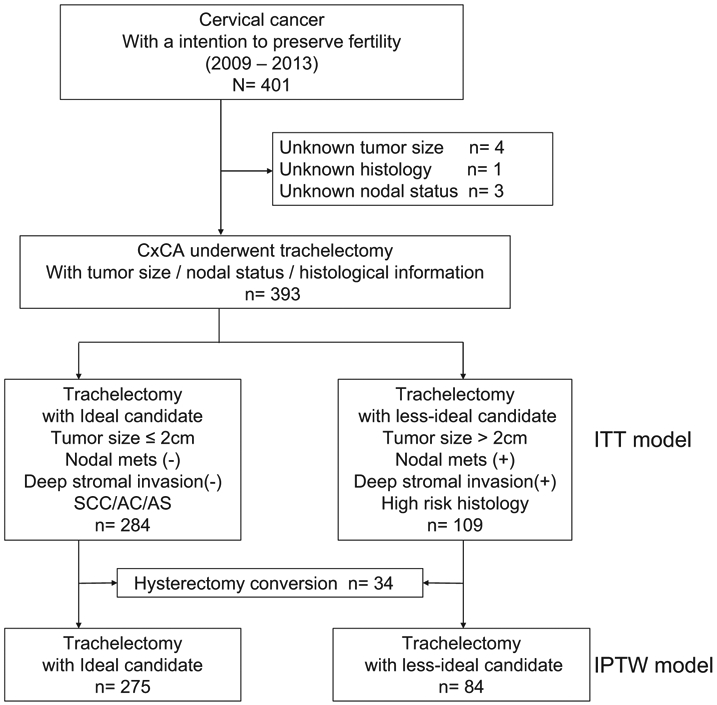
Methods: This nationwide, multicenter, retrospective study was conducted by the Japan Society of Obstetrics and Gynecology involving women aged <45 years with clinical stage I-II cervical cancer who had planned fertility-sparing trachelectomy and pelvic lymphadenectomy between 2009 and 2013 (n = 393). Ideal candidates were defined to have a tumor size of ≤2 cm, no lymph node metastasis, no deep stromal invasion, and no high-risk histology (n = 284, 69.6%). Less-ideal candidates were defined to have any one of these four characteristics (n = 109, 30.4%). Propensity score inverse probability of treatment weighting was used to assess survival outcomes.
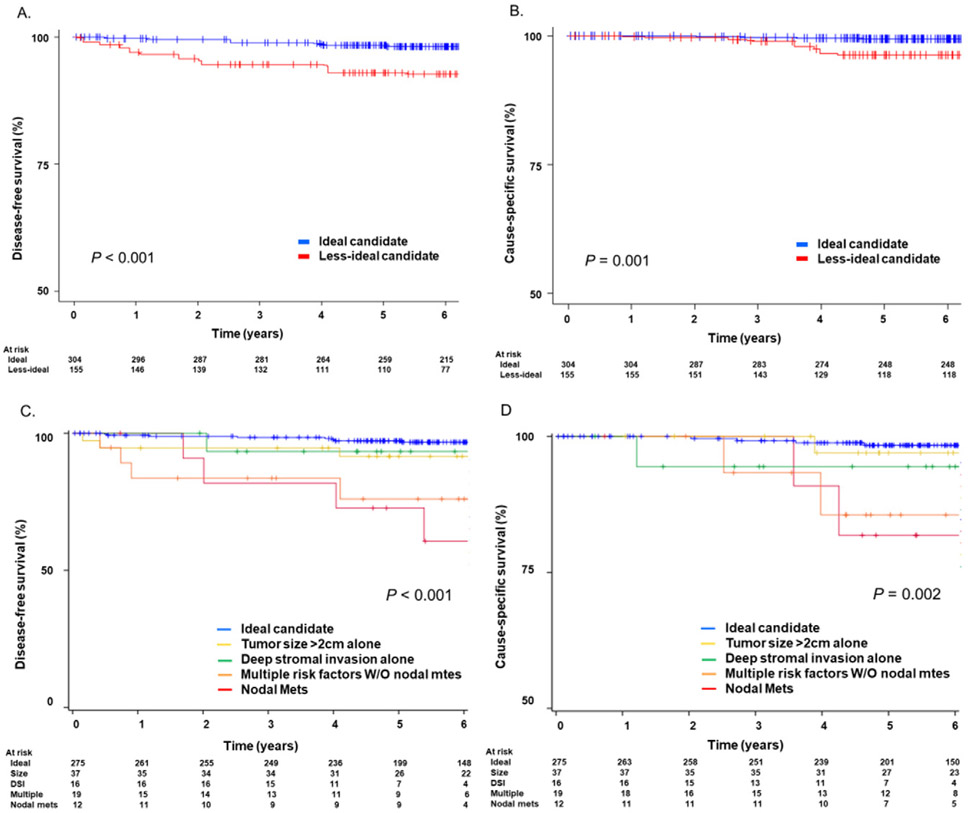
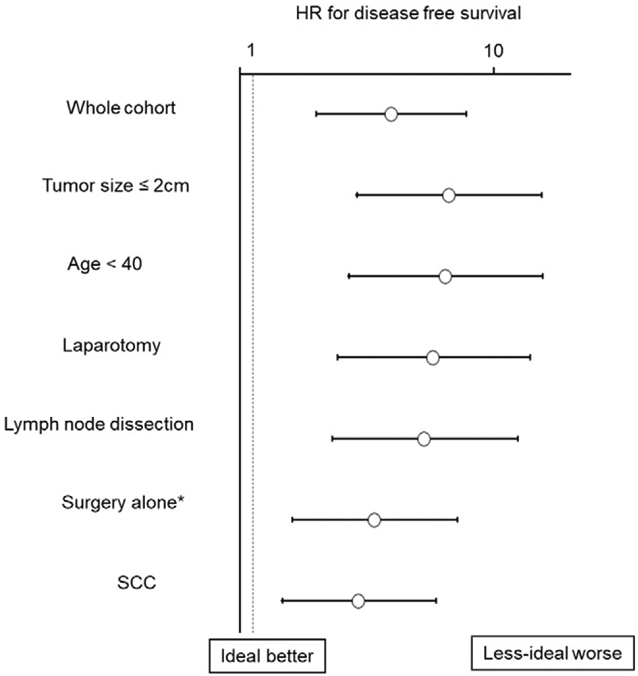
Results: Less-ideal candidates were more likely to undergo hysterectomy conversion (22.9% versus 3.2%), receive postoperative radiotherapy (11.9% versus 0.4%), or chemotherapy (32.1% versus 3.2%) compared with ideal candidates (all, P < 0.05). The weighted model revealed that among those who underwent trachelectomy (ideal candidates, n = 275 and less-ideal candidates, n = 84), less-ideal candidates had significantly decreased disease-free survival (5-year rates: 85.5% versus 95.5%; HR 3.93, 95% CI 1.99-7.74; P < 0.001) and cause-specific survival (92.5% versus 98.6%; HR 5.47, 95% CI 1.68-17.8, P = 0.001) compared with ideal candidates. Similarly, less-ideal candidates were significantly associated with decreased disease-free survival compared with ideal candidates among those who were young age, had small tumors or squamous histology, and underwent surgery alone (all, P < 0.05).
Conclusion: Less-ideal candidates had approximately four-fold higher recurrence risk and cancer mortality compared with ideal candidates. Ideal candidates for fertility-sparing trachelectomy for early-stage cervical cancer proposed in our study may be useful as the future framework for developing guidelines for fertility-sparing trachelectomy in Japan.
Keywords: Cervical cancer; Deep stromal invasion; Lymph node metastasis; Survival; Trachelectomy; Tumor size.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The validity of the subsequent pregnancy index score for fertility-sparing trachelectomy in early-stage cervical cancer.Fertil Steril. 2021 May;115(5):1250-1258. doi: 10.1016/j.fertnstert.2020.09.162. Epub 2021 Feb 13. Fertil Steril. 2021. PMID: 33589139
-
Fertility sparing therapy in women with lymph node negative cervical cancer >2cm - oncologic and fertility outcomes of neoadjuvant chemotherapy followed by radical vaginal trachelectomy.Int J Gynecol Cancer. 2023 Oct 2;33(10):1542-1547. doi: 10.1136/ijgc-2023-004669. Int J Gynecol Cancer. 2023. PMID: 37696645
-
Radical Trachelectomy for Early Stage Cervical Cancer.Curr Treat Options Oncol. 2018 Nov 19;19(12):75. doi: 10.1007/s11864-018-0591-4. Curr Treat Options Oncol. 2018. PMID: 30450531 Review.
-
Trends in Use and Survival Associated With Fertility-Sparing Trachelectomy for Young Women With Early-Stage Cervical Cancer.Obstet Gynecol. 2018 Jun;131(6):1085-1094. doi: 10.1097/AOG.0000000000002613. Obstet Gynecol. 2018. PMID: 29742670 Free PMC article.
-
Less radical surgery for early-stage cervical cancer: To what extent do we justify it?-Our belief.Taiwan J Obstet Gynecol. 2016 Aug;55(4):495-8. doi: 10.1016/j.tjog.2016.01.004. Taiwan J Obstet Gynecol. 2016. PMID: 27590369 Review.
Cited by
-
Adoption strategies of fertility-sparing surgery for early-stage cervical cancer patients based on clinicopathological characteristics: a large retrospective cohort study.Front Surg. 2024 Aug 22;11:1456376. doi: 10.3389/fsurg.2024.1456376. eCollection 2024. Front Surg. 2024. PMID: 39239473 Free PMC article.
-
Fertility-Sparing Surgery in Gynecologic Cancer: A Systematic Review.Cancers (Basel). 2021 Feb 28;13(5):1008. doi: 10.3390/cancers13051008. Cancers (Basel). 2021. PMID: 33670929 Free PMC article. Review.
-
Cervical Cancer and Fertility-Sparing Treatment.J Clin Med. 2021 Oct 21;10(21):4825. doi: 10.3390/jcm10214825. J Clin Med. 2021. PMID: 34768345 Free PMC article. Review.
-
Fertility-Sparing and Less Radical Surgery for Cervical Cancer.Curr Oncol Rep. 2022 Nov;24(11):1541-1548. doi: 10.1007/s11912-022-01317-w. Epub 2022 Aug 12. Curr Oncol Rep. 2022. PMID: 35953599 Free PMC article. Review.
-
Fertility Preservation in Cervical Cancer-Treatment Strategies and Indications.Curr Oncol. 2024 Jan 4;31(1):296-306. doi: 10.3390/curroncol31010019. Curr Oncol. 2024. PMID: 38248104 Free PMC article. Review.
References
-
- Projected Cancer Statistics, Cancer information service, https://ganjoho.jp/en/public/statistics/short_pred.html, 2018. Accessed date: 4 September 2019.
-
- Peters WA 3rd, Liu PY, Barrett RJ 2nd, Stock RJ, Monk BJ, Berek JS, et al., Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix, J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol 18 (2000) 1606–1613. - PubMed
-
- Monk BJ, Wang J, Im S, Stock RJ, Peters WA 3rd, Liu PY, et al., Rethinking the use of radiation and chemotherapy after radical hysterectomy: a clinical-pathologic analysis of a Gynecologic Oncology Group/Southwest Oncology Group/Radiation Therapy Oncology Group trial, Gynecol. Oncol 96 (2005) 721–728. - PubMed
-
- Querleu D, Morrow CP, Classification of radical hysterectomy, Lancet Oncol. 9 (2008) 297–303. - PubMed
-
- Cervical cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines), https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf, Accessed date: 20 August 2019.
