

A randomised assessment of image guided radiotherapy within a phase 3 trial of conventional or hypofractionated high dose intensity modulated radiotherapy for prostate cancer
- PMID: 31767473
- PMCID: PMC7005673
- DOI: 10.1016/j.radonc.2019.10.017
A randomised assessment of image guided radiotherapy within a phase 3 trial of conventional or hypofractionated high dose intensity modulated radiotherapy for prostate cancer
Abstract
Background and purpose: Image-guided radiotherapy (IGRT) improves treatment set-up accuracy and provides the opportunity to reduce target volume margins. We introduced IGRT methods using standard (IGRT-S) or reduced (IGRT-R) margins in a randomised phase 2 substudy within CHHiP trial. We present a pre-planned analysis of the impact of IGRT on dosimetry and acute/late pelvic side effects using gastrointestinal and genitourinary clinician and patient-reported outcomes (PRO) and evaluate efficacy.
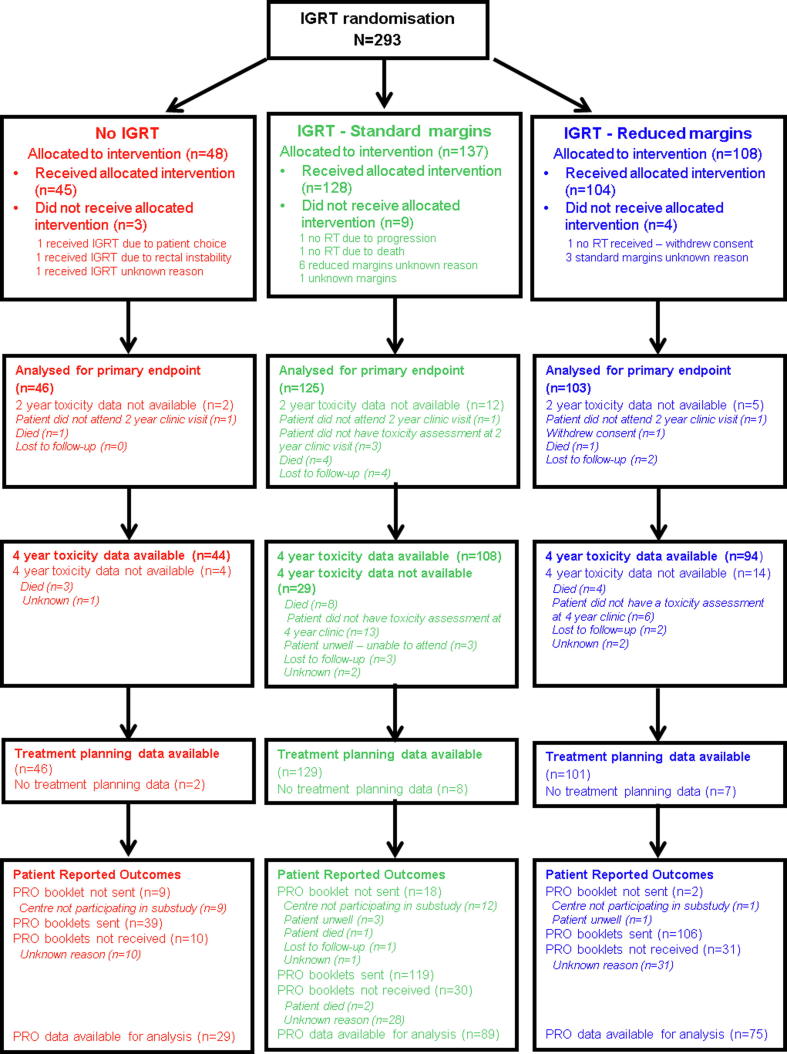
Materials and methods: CHHiP is a randomised phase 3, non-inferiority trial for men with localised prostate cancer. 3216 patients were randomly assigned to conventional (74 Gy in 2 Gy/fraction (f) daily) or moderate hypofractionation (60 or 57 Gy in 3 Gy/f daily) between October 2002 and June 2011. The IGRT substudy included a second randomisation assigning to no-IGRT, IGRT-S (standard CTV-PTV margins), or IGRT-R (reduced CTV-PTV margins). Primary substudy endpoint was late RTOG bowel and urinary toxicity at 2 years post-radiotherapy.
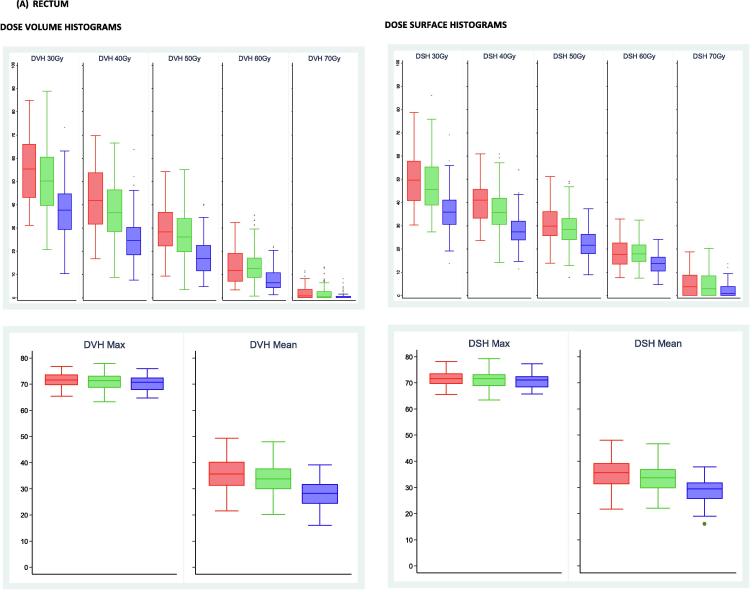
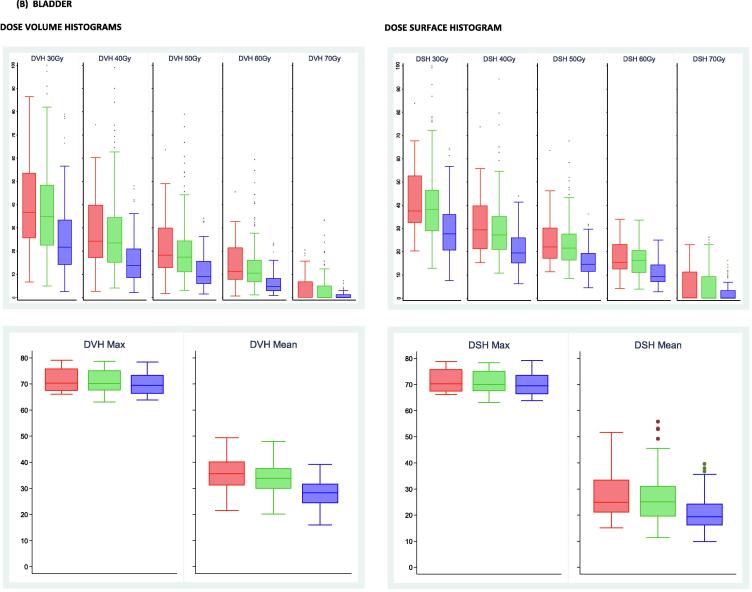
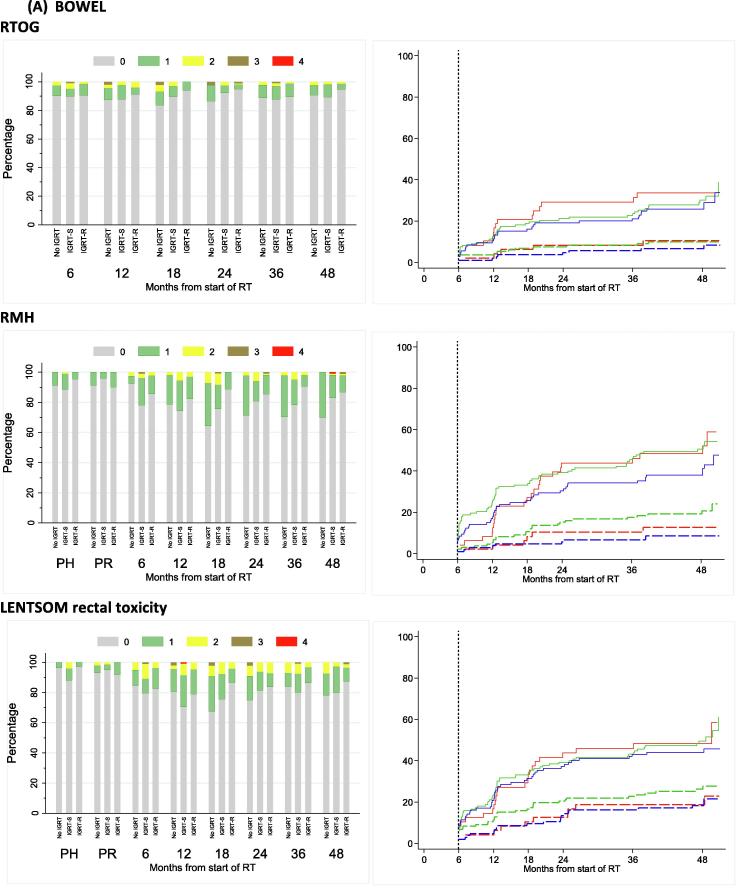
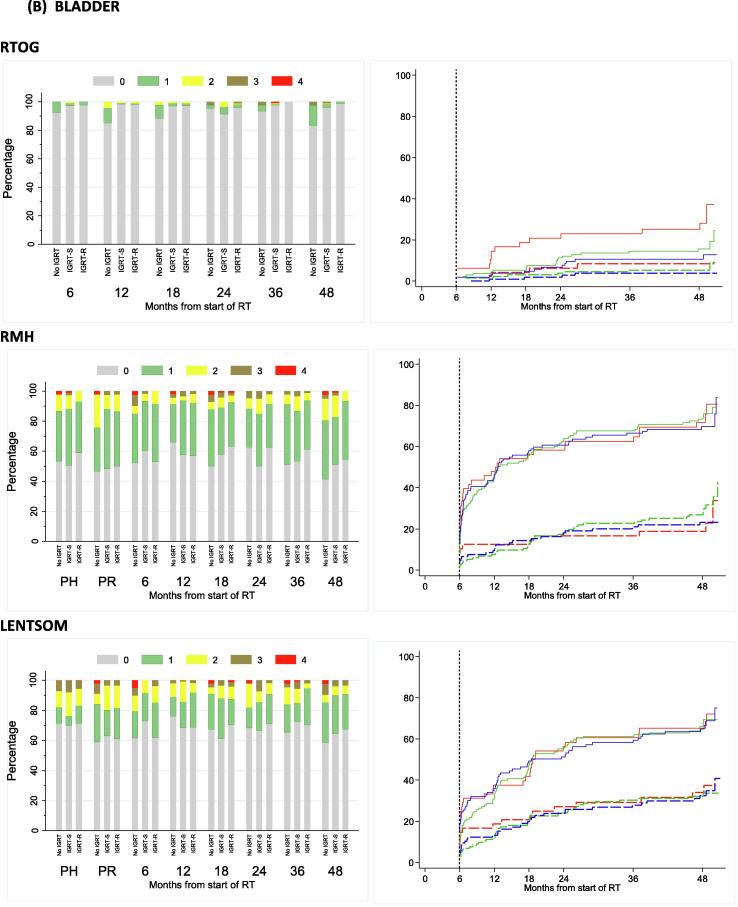
Results: Between June 2010 to July 2011, 293 men were recruited from 16 centres. Median follow-up is 56.9(IQR 54.3-60.9) months. Rectal and bladder dose-volume and surface percentages were significantly lower in IGRT-R compared to IGRT-S group; (p < 0.0001). Cumulative proportion with RTOG grade ≥ 2 toxicity reported to 2 years for bowel was 8.3(95% CI 3.2-20.7)%, 8.3(4.7-14.6)% and 5.8(2.6-12.4)% and for urinary 8.4(3.2-20.8)%, 4.6(2.1-9.9)% and 3.9(1.5-9.9)% in no IGRT, IGRT-S and IGRT-R groups respectively. In an exploratory analysis, treatment efficacy appeared similar in all three groups.
Conclusion: Introduction of IGRT was feasible in a national randomised trial and IGRT-R produced dosimetric benefits. Overall side effect profiles were acceptable in all groups but lowest with IGRT and reduced margins.
Isrctn: 97182923.
Keywords: Dosimetry; Image-guided radiotherapy; Prostate; Toxicity.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- Pollack A., Zagars G.K., Starkschall G., Antolak J.A., Lee J.J., Huang E. Prostate cancer radiation dose response: results of the M. D. Anderson phase III randomized trial. Int J Radiat Oncol Biol Phys. 2002;53(5):1097–1105. - PubMed
-
- Zietman A.L., DeSilvio M.L., Slater J.D., Rossi C.J., Jr., Miller D.W., Adams J.A. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA. 2005;294(10):1233–1239. - PubMed
-
- Zelefsky M.J., Yamada Y., Kollmeier M.A., Shippy A.M., Nedelka M.A. Long-term outcome following three-dimensional conformal/intensity-modulated external-beam radiotherapy for clinical stage T3 prostate cancer. Eur Urol. 2008;53(6):1172–1179. - PubMed
-
- Al-Mamgani A., Heemsbergen W.D., Peeters S.T., Lebesque J.V. Role of intensity-modulated radiotherapy in reducing toxicity in dose escalation for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2009;73(3):685–691. - PubMed
-
- McNair H.A., Hansen V.N., Parker C.C., Evans P.M., Norman A., Miles E. A comparison of the use of bony anatomy and internal markers for offline verification and an evaluation of the potential benefit of online and offline verification protocols for prostate radiotherapy. Int J Radiat Oncol Biol Phys. 2008;71(1):41–50. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
