

Predictors of Mortality in Bloodstream Infections Caused by Pseudomonas aeruginosa and Impact of Antimicrobial Resistance and Bacterial Virulence
- PMID: 31767719
- PMCID: PMC6985728
- DOI: 10.1128/AAC.01759-19
Predictors of Mortality in Bloodstream Infections Caused by Pseudomonas aeruginosa and Impact of Antimicrobial Resistance and Bacterial Virulence
Abstract
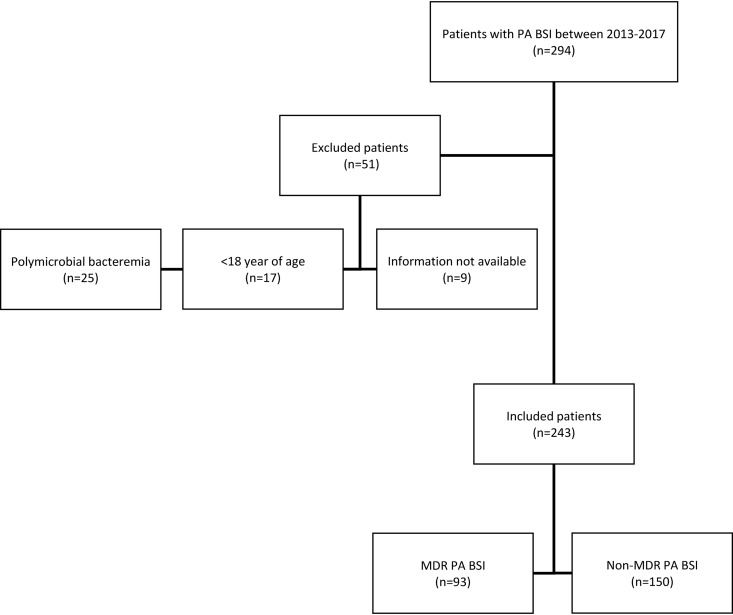
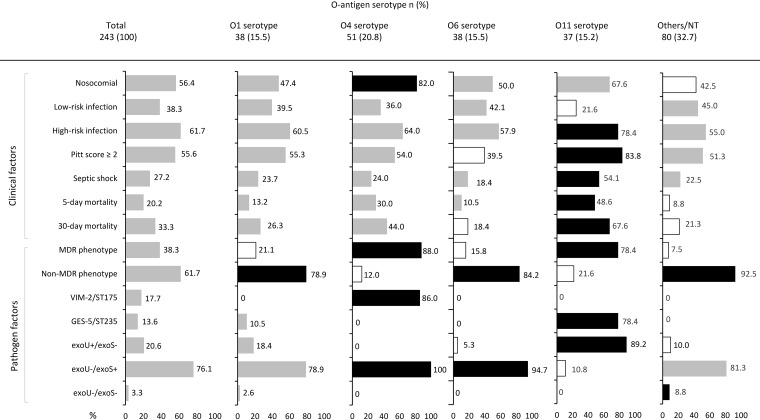
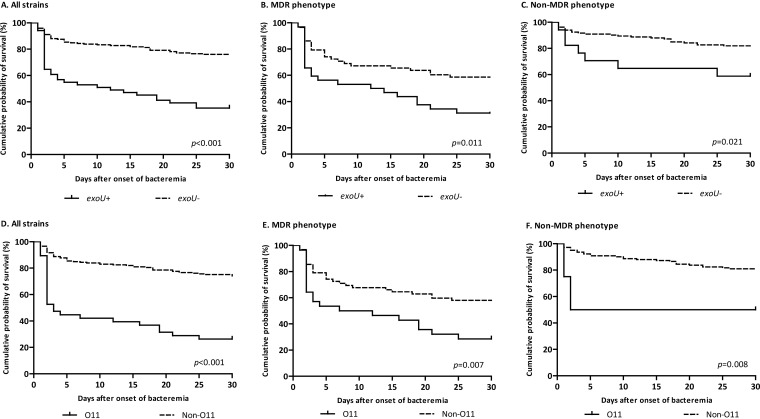
Whether multidrug resistance (MDR) is associated with mortality in patients with Pseudomonas aeruginosa bloodstream infections (BSI) remains controversial. Here, we explored the prognostic factors of P. aeruginosa BSI with emphasis on antimicrobial resistance and virulence. All P. aeruginosa BSI episodes in a 5-year period were retrospectively analyzed. The impact in early (5-day) and late (30-day) crude mortality of host, antibiotic treatment, and pathogen factors was assessed by multivariate logistic regression analysis. Of 243 episodes, 93 (38.3%) were caused by MDR-PA. Crude 5-day (20%) and 30-day (33%) mortality was more frequent in patients with MDR-PA (34.4% versus 11.3%, P < 0.001 and 52.7% versus 21.3%, P < 0.001, respectively). Early mortality was associated with neutropenia (adjusted odds ratio [aOR], 9.21; 95% confidence interval [CI], 3.40 to 24.9; P < 0.001), increased Pitt score (aOR, 2.42; 95% CI, 1.34 to 4.36; P = 0.003), respiratory source (aOR, 3.23; 95% CI,2.01 to 5.16; P < 0.001), inadequate empirical therapy (aOR, 4.57; 95% CI, 1.59 to 13.1; P = 0.005), shorter time to positivity of blood culture (aOR, 0.88; 95% CI, 0.80 to 0.97; P = 0.010), an exoU-positive genotype (aOR, 3.58; 95% CI, 1.31 to 9.79; P = 0.013), and the O11 serotype (aOR, 3.64; 95% CI, 1.20 to 11.1; P = 0.022). These risk factors were similarly identified for late mortality, along with an MDR phenotype (aOR, 2.18; 95% CI, 1.04 to 4.58; P = 0.040). Moreover, the O11 serotype (15.2%, 37/243) was common among MDR (78.4%, 29/37) and exoU-positive (89.2%, 33/37) strains. Besides relevant clinical variables and inadequate empirical therapy, pathogen-related factors such as an MDR phenotype, an exoU-positive genotype, and the O11 serotype adversely affect the outcome of P. aeruginosa BSI.
Keywords: Pseudomonas aeruginosa; antimicrobial resistance; bloodstream infections; mortality; virulence.
Copyright © 2020 American Society for Microbiology.
Figures
References
-
- Peña C, Suarez C, Gozalo M, Murillas J, Almirante B, Pomar V, Aguilar M, Granados A, Calbo E, Rodríguez-Baño J, Rodríguez F, Tubau F, Martínez-Martínez L, Oliver A. 2012. Prospective multicenter study of the impact of carbapenem resistance on mortality in Pseudomonas aeruginosa bloodstream infections. Antimicrob Agents Chemother 56:1265–1272. doi:10.1128/AAC.05991-11. - DOI - PMC - PubMed
-
- Peña C, Suarez C, Ocampo-Sosa A, Murillas J, Almirante B, Pomar V, Aguilar M, Granados A, Calbo E, Rodríguez-Baño J, Rodríguez F, Tubau F, Oliver A, Martínez-Martínez L. 2013. Effect of adequate single-drug vs combination antimicrobial therapy on mortality in Pseudomonas aeruginosa bloodstream infections: a post hoc analysis of a prospective cohort. Clin Infect Dis 57:208–216. doi:10.1093/cid/cit223. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
