

Activating mutations in CSF1R and additional receptor tyrosine kinases in histiocytic neoplasms
- PMID: 31768065
- PMCID: PMC6898787
- DOI: 10.1038/s41591-019-0653-6
Activating mutations in CSF1R and additional receptor tyrosine kinases in histiocytic neoplasms
Abstract
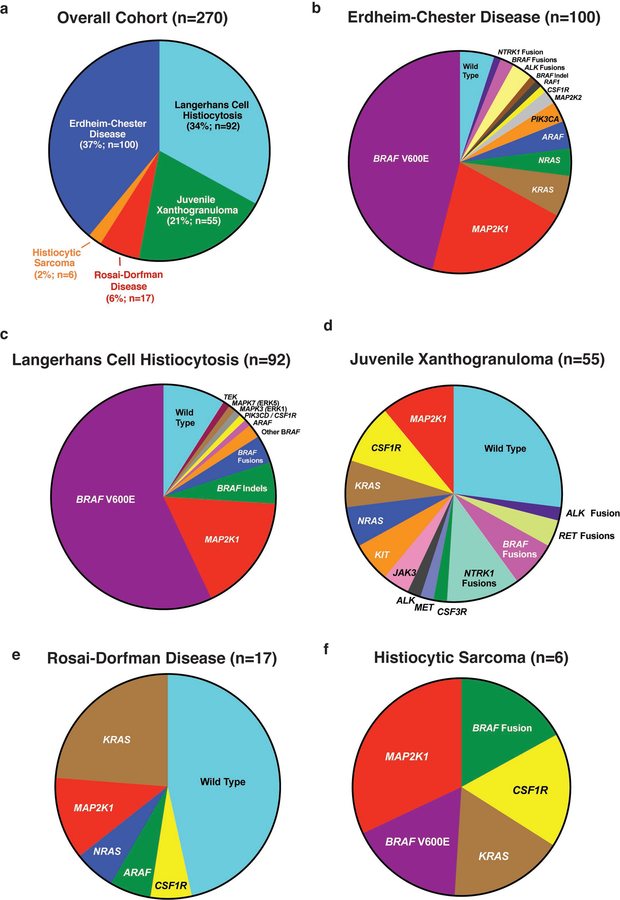
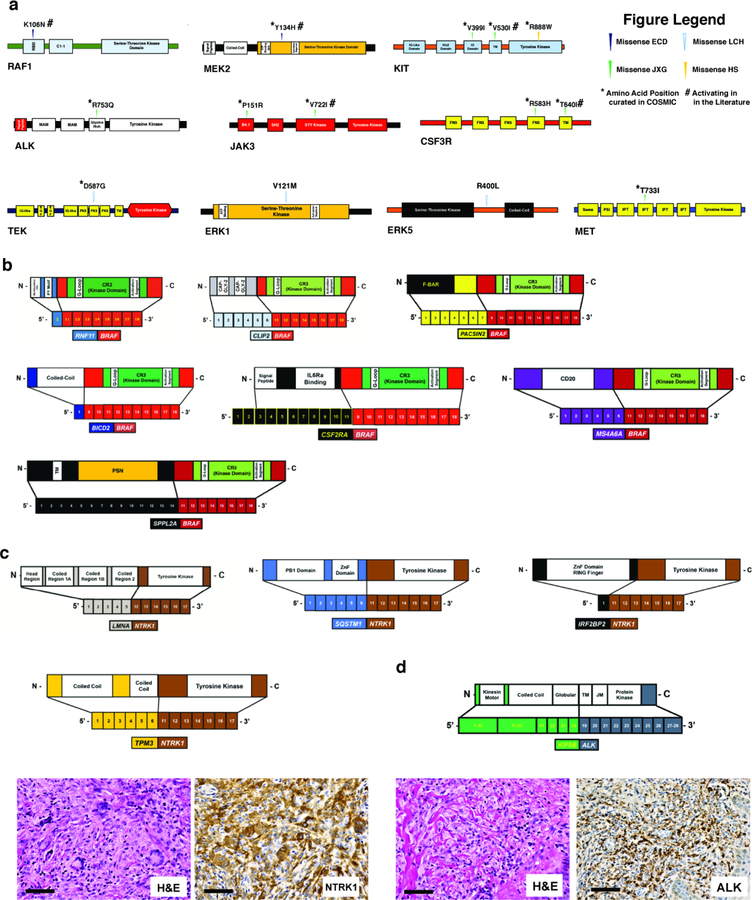
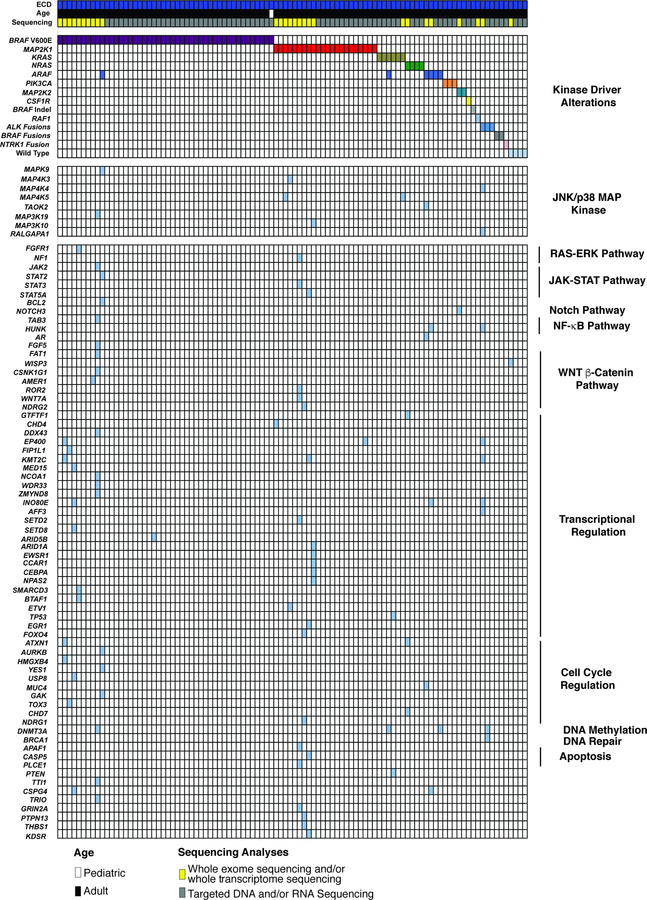
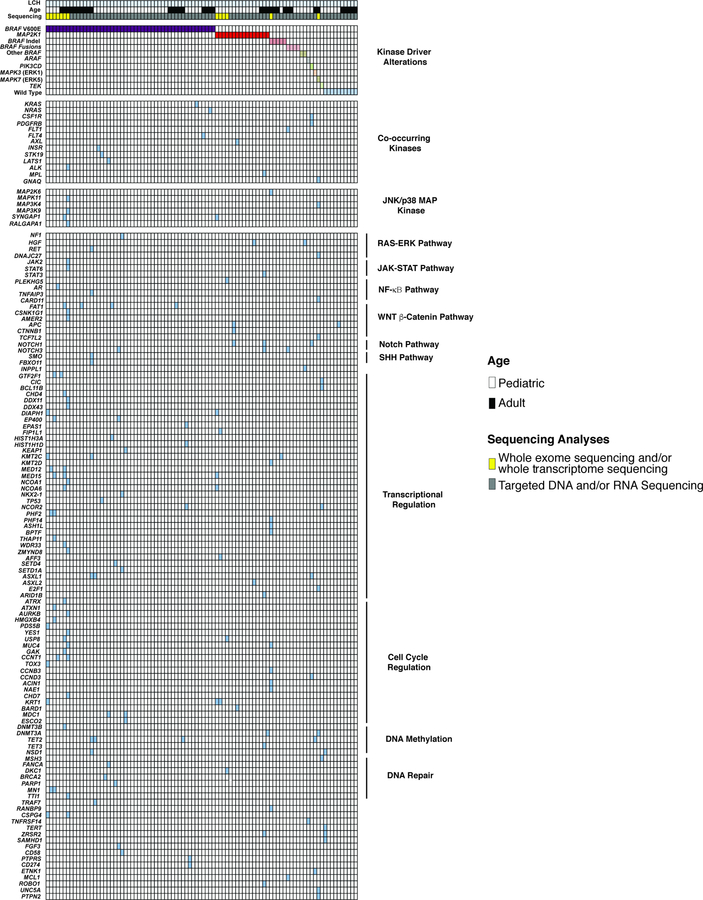
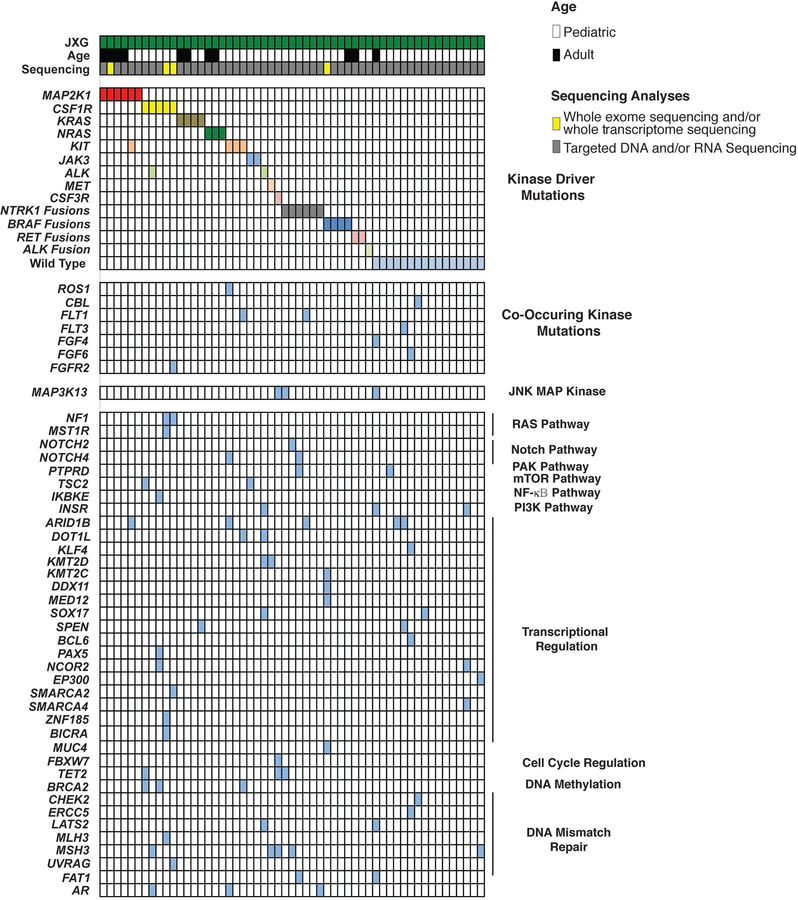
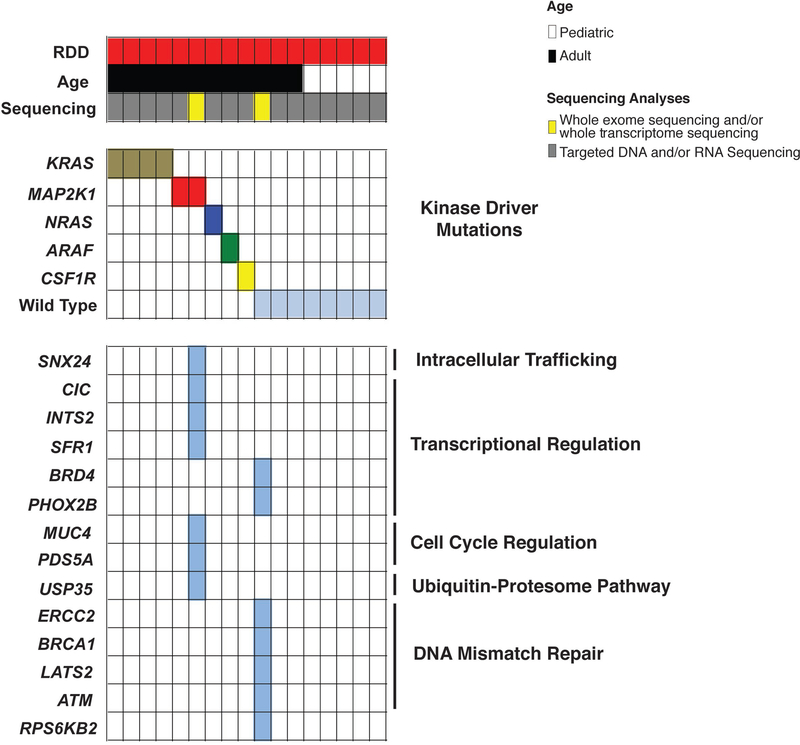
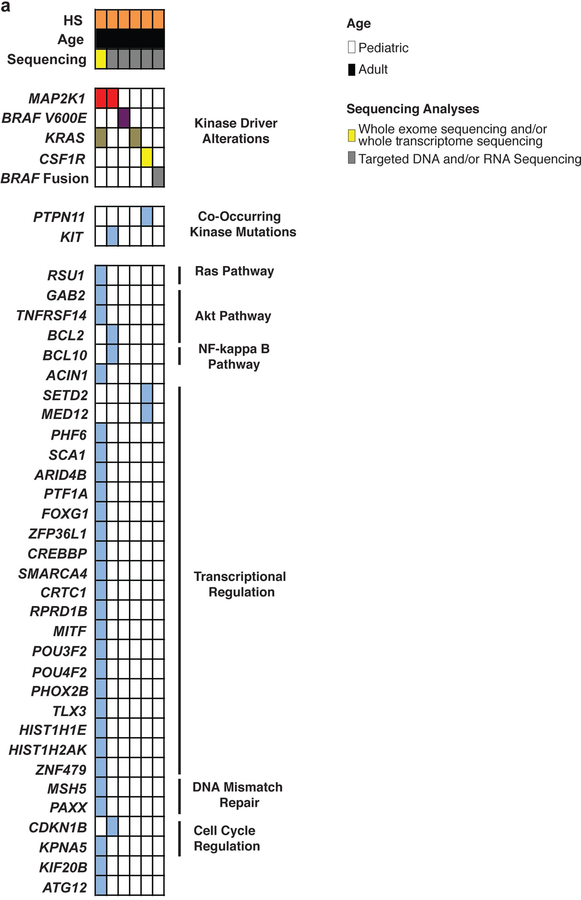
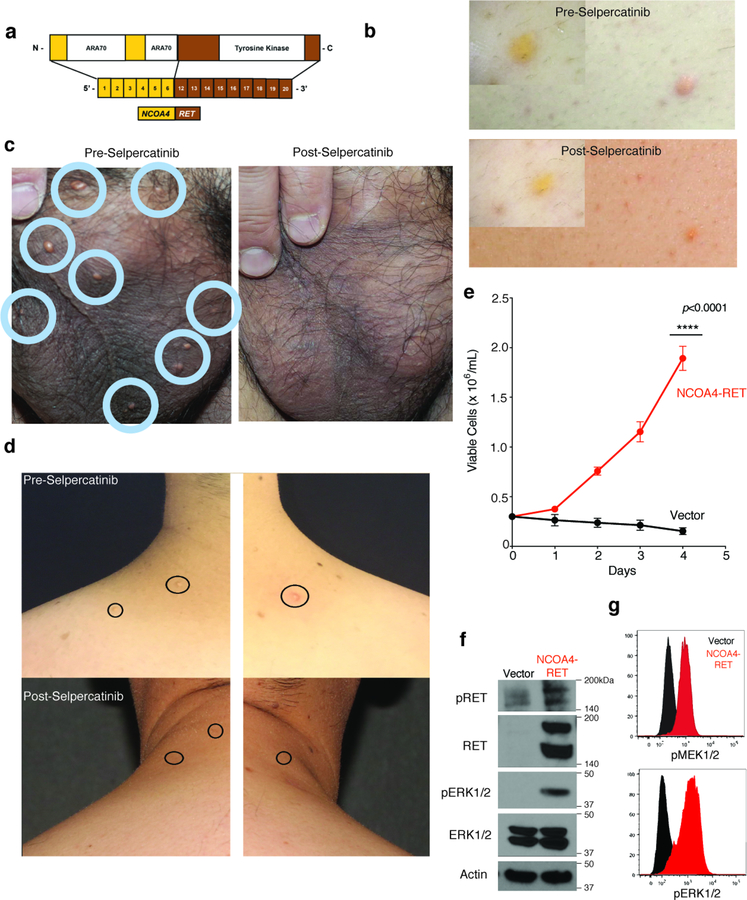
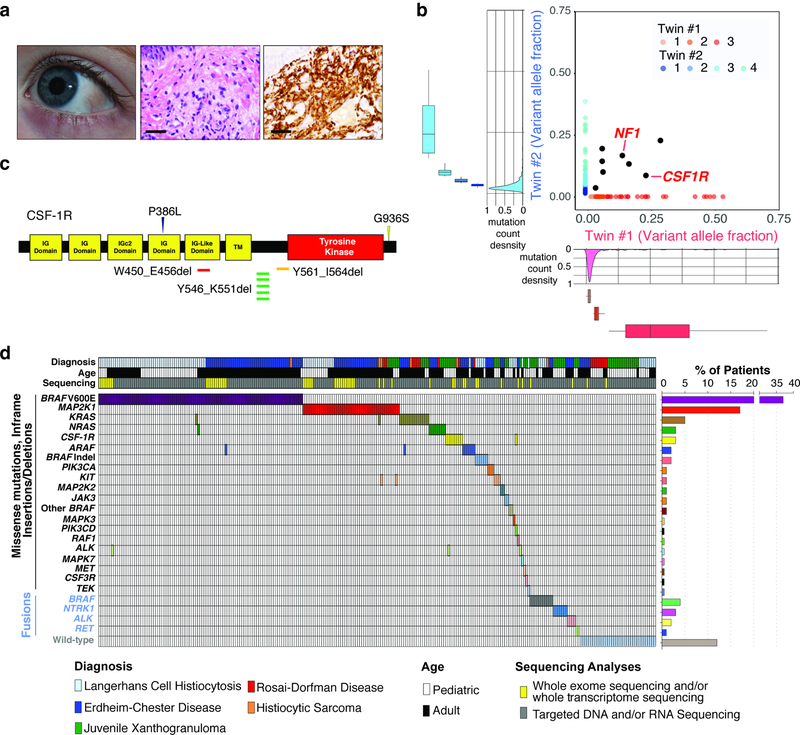
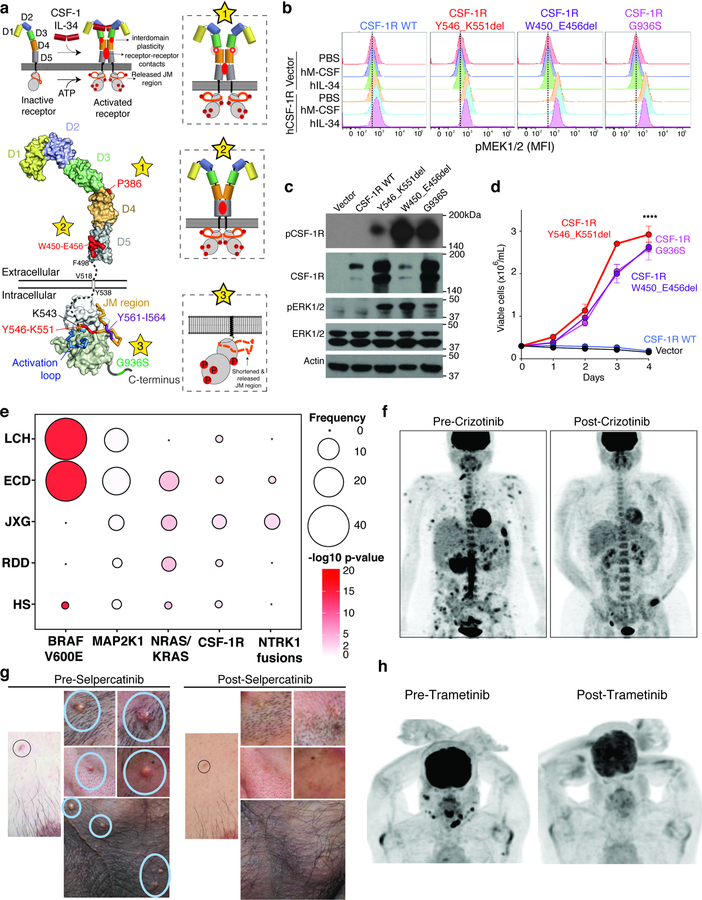
Histiocytoses are clonal hematopoietic disorders frequently driven by mutations mapping to the BRAF and MEK1 and MEK2 kinases. Currently, however, the developmental origins of histiocytoses in patients are not well understood, and clinically meaningful therapeutic targets outside of BRAF and MEK are undefined. In this study, we uncovered activating mutations in CSF1R and rearrangements in RET and ALK that conferred dramatic responses to selective inhibition of RET (selpercatinib) and crizotinib, respectively, in patients with histiocytosis.
Conflict of interest statement
Competing financial interests
The authors declare the following competing interests: B.H.D.: grants from National Cancer Institute, American Society of Hematology, and Erdheim-Chester Disease Global Alliance Foundation. A.Y.: grants from the Leukemia & Lymphoma Society, Aplastic Anemia & MDS International Foundation, and the Lauri Strauss Leukemia Foundation. G.A.U.: personal fees from Sanofi and grants from Sanofi, Novartis, Genentech. M. Ladanyi: advisory board compensation from Merck, AstraZeneca, BristolMyers Squibb, Takeda, and Bayer, and research support from LOXO Oncology and Helsinn Healthcare. D.B.S.: served as a consultant and received honoraria from Pfizer, Loxo Oncology, Lilly Oncology, Vivideon Therapeutics and Illumina. Stock options from Loxo Oncology. M.F.B.: personal fees from Roche and research support from Illumina. D.M.H.: personal fees from Atara Biotherapeutics, Chugai Pharma, Boehringer Ingelheim, AstraZeneca, Pfizer, Bayer, Debiopharm Group, and Genentech, and grants from National Cancer Institute, AstraZeneca, Puma Biotechnology, and Loxo Oncology. I.D.: served as a consultant for Apexigen, Bayer, and Celgene and research support from BMS and Novartis. S.N.S.: program grants from the Flanders Institute for Biotechnology, Belgium (VIB) and the special research fund of Ghent University, and grants for Research Foundation Flanders (FWO). M.E.L.: personal fees from LOXO, AstraZeneca, Roche/Genentech, Novartis. AD: Research fuding from Foundation Medicine and personal fees from Ignyta/Genentech/Roche, Loxo/Bayer/Lilly, Takeda/Ariad/Millenium, TP Therapeutics, AstraZeneca, Pfizer, Blueprint Medicines, Helsinn, Beigene, BergenBio, Hengrui Therapeutics, Exelixis, Tyra Biosciences, Verastem, and MORE Health. E.L.D.: grants from Erdheim-Chester Disease Global Alliance, The Histiocytosis Association, the Society of Memorial Sloan Kettering, the Frame Fund, the Joy Family West Foundation, and the American Society for Clinical Oncology. O.A.-W.: grants from National Cancer Institute, National Heart Lung and Blood Institute, Pershing Square Sohn Foundation, the Histiocyte Society, and H3B Biomedicine, and personal fees from H3B Biomedicine, Foundation Medicine Inc., Merck, and Jansen unrelated to this manuscript. The remaining authors have nothing to disclose.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
