

Parafalcine subdural empyema: The unresolved controversy over the need for surgical treatment
- PMID: 31768283
- PMCID: PMC6826320
- DOI: 10.25259/SNI_392_2019
Parafalcine subdural empyema: The unresolved controversy over the need for surgical treatment
Abstract
Background: Parafalcine subdural empyema (SDE) is a rare entity consisting of pus accumulating below the longitudinal sinus, between the falx cerebri and the arachnoid layer covering the medial surface of the cerebral hemisphere. Its treatment strategy is controversial, but most clinicians have the general belief that appropriate treatment consists of prompt surgery combined with long-term antibiotic therapy. Nevertheless, six reports published in the 1980s provided evidence that antibiotic therapy alone is a safe and suitable option. The treatment strategies and outcomes of the 31 well-described cases previously published, in addition to our own, are discussed.
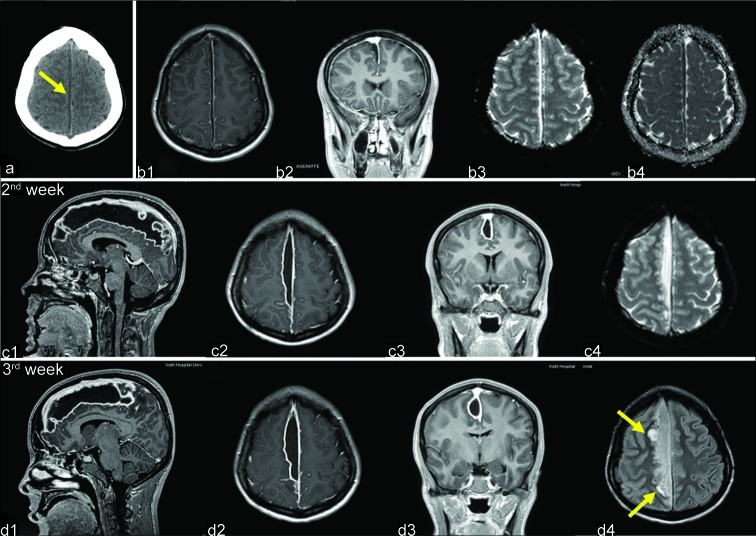
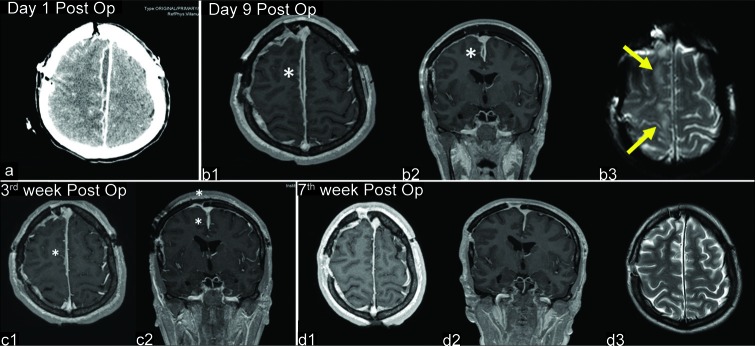
Case description: We report a 21-year-old female with a right-side parafalcine SDE who presented with fever, headache, generalized tonic-clonic seizures, and contralateral hemiparesis 3 weeks after undergoing sinonasal surgery. Despite clinical symptoms almost entirely abating after starting treatment with broad-spectrum antibiotics, magnetic resonance imaging performed during the 2nd and 3rd weeks showed progressive enlargement of the interhemispheric collection (from 4 cm3 to 30 cm3). We reflect on the treatment strategy chosen for this patient, who experienced a total recovery.
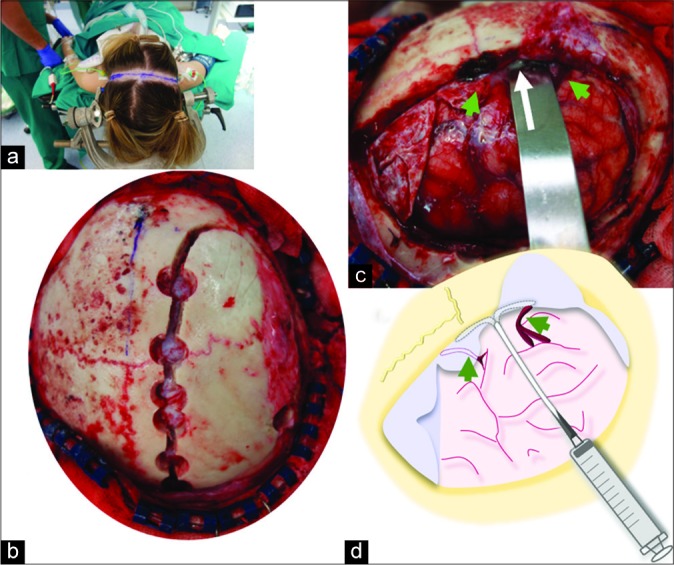
Conclusion: A nonsurgical strategy for parafalcine SDE might be contemplated for patients with a good clinical condition and no major midline shift on neuroradiological studies, given their usual indolent course and the relative difficulty in reaching the interhemispheric fissure. Conversely, surgery should be contemplated when the collection significantly enlarges despite antibiotic therapy. When surgical drainage is added to antibiotics, broad- range 16S ribosomal DNA polymerase chain reaction of the empyema is recommended to identify the causative organism as pus cultures are usually sterile.
Keywords: 16S ribosomal DNA polymerase chain reaction; Antibiotic therapy; Interhemispheric empyema; Parafalcine subdural empyema; Surgery.
Copyright: © 2019 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Akhaddar A, editor. Atlas of Infections in Neurosurgery and Spinal Surgery. 1st ed. Switzerland: Springer International Publishing; 2017. Cranial subdural empyemas; pp. 51–64.
-
- Arifianto MR, Ma’ruf AZ, Ibrahim A, Bajamal AH. Interhemispheric and infratentorial subdural empyema with preseptal cellulitis as complications of sinusitis: A case report. Pediatr Neurosurg. 2018;53:128–33. - PubMed
-
- Baerlocher K, Arregger G, Benini A, Gaspar B, Valavanis A, Schubiger O, et al. Subdural interhemispheric empyema in a 7-year-old boy. Helv Paediatr Acta. 1979;34:583–8. - PubMed
-
- Bok AP, Peter JC. Subdural empyema: Burr holes or craniotomy? A retrospective computerized tomography-era analysis of treatment in 90 cases. J Neurosurg. 1993;78:574–8. - PubMed
-
- Borovich B, Braun J, Honigman S, Joachims HZ, Peyser E. Supratentorial and parafalcial subdural empyema diagnosed by computerized tomography. Case report. J Neurosurg. 1981;54:105–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous