

Chiari malformation and types of basilar invagination with/without syringomyelia
- PMID: 31768286
- PMCID: PMC6826318
- DOI: 10.25259/SNI_469_2019
Chiari malformation and types of basilar invagination with/without syringomyelia
Abstract
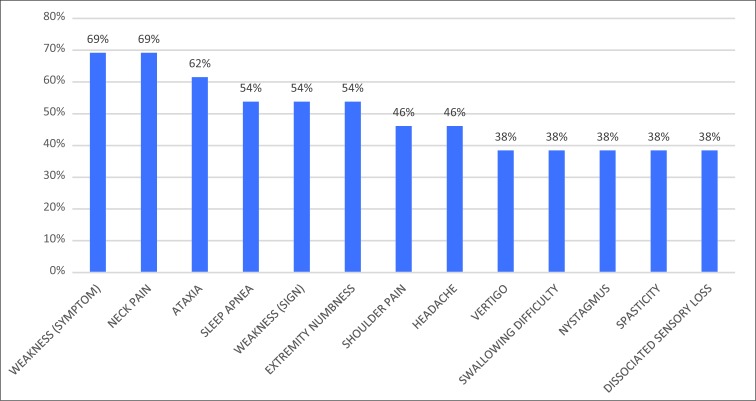
Background: Craniometric studies document different subtypes of craniocervical junction malformations (CCJM). Here, we identified the different types and global signs and symptoms (SS) that correlated with these malformations while further evaluating the impact of syringomyelia.
Methods: Prospective data concerning SS and types of CCJM were evaluated in 89 patients between September 2002 and April 2014 using Bindal's scale.
Results: The mean Bindal's scores of each type of CCJM were Chiari malformation (CM) = 74.6, basilar invagination Type 1 (BI1) = 78.5, and BI Type 2 (BI2) = 78. Swallowing impairment and nystagmus were more frequently present in the BI patients. Symptomatic burdens were higher in patients with syringomyelia and included weakness, extremity numbness, neck pain, dissociated sensory loss, and atrophy.
Conclusion: There were no statistically significant differences in SS between the different CCJM types. BI patients had more swallowing and nystagmus complaints versus CM patients, but there were no significant differences in clinical SS between BI1 and BI2 patients. Notably, those with attendant syringomyelia had a higher SS burden.
Keywords: Arnold–Chiari malformation; Basilar impression; Neurologic manifestations; Platybasia; Signs and symptoms.
Copyright: © 2019 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- Bindal AK, Dunsker SB, Tew JM., Jr Chiari I malformation: Classification and management. Neurosurgery. 1995;37:1069–74. - PubMed
-
- Botelho RV, Diniz JM. Basilar Invagination: Cranio-cervical kyphosis rather than prolapse from the upper cervical spine. J Neurol Neuromed. 2017;2:15–9.
-
- Goel A. Basilar invagination, chiari malformation, syringomyelia: A review. Neurol India. 2009;57:235–46. - PubMed
-
- Guerreiro RB, Bittencourt L, Reis RC, Rotta JM, Tufik S, Botelho RV, et al. Upper airway dimensions in patients with craniocervical junction malformations with and without sleep apnea. A pilot case-control study. Arq Neuropsiquiatr. 2015;73:336–41. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous