

Intraoperative Oxidative Damage and Delirium after Cardiac Surgery
- PMID: 31770146
- PMCID: PMC7015795
- DOI: 10.1097/ALN.0000000000003016
Intraoperative Oxidative Damage and Delirium after Cardiac Surgery
Abstract
Background: Mechanisms of postoperative delirium remain poorly understood, limiting development of effective treatments. We tested the hypothesis that intraoperative oxidative damage is associated with delirium and neuronal injury and that disruption of the blood-brain barrier modifies these associations.
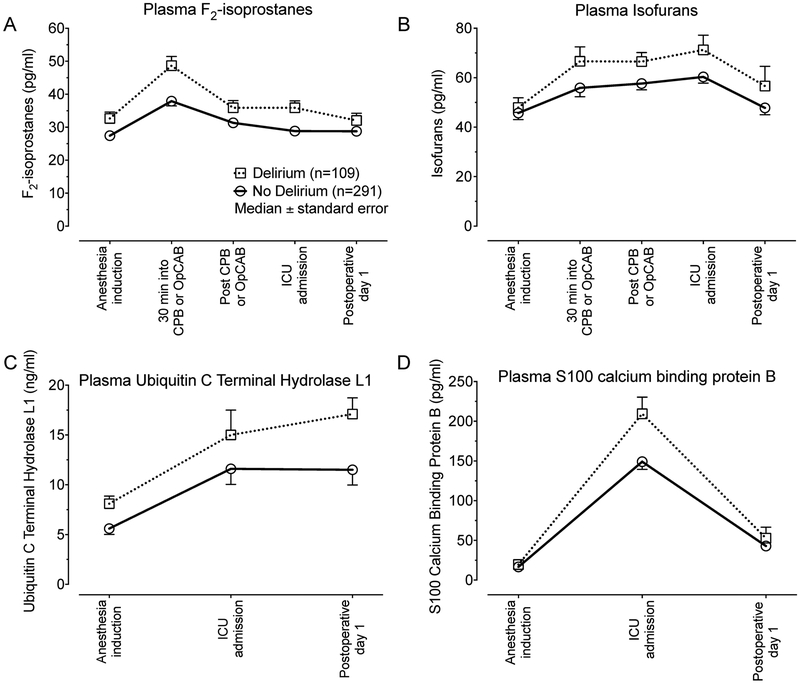
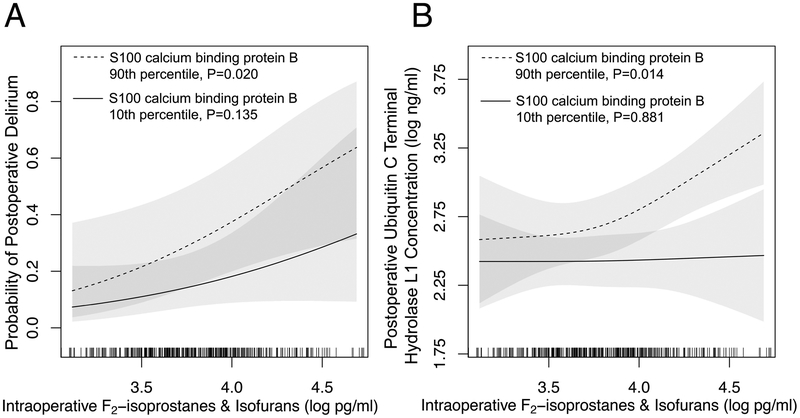
Methods: In a prespecified cohort study of 400 cardiac surgery patients enrolled in a clinical trial of atorvastatin to reduce kidney injury and delirium, we measured plasma concentrations of F2-isoprostanes and isofurans using gas chromatography-mass spectrometry to quantify oxidative damage, ubiquitin carboxyl-terminal hydrolase isozyme L1 to quantify neuronal injury, and S100 calcium-binding protein B using enzyme-linked immunosorbent assays to quantify blood-brain barrier disruption before, during, and after surgery. We performed the Confusion Assessment Method for the Intensive Care Unit twice daily to diagnose delirium. We measured the independent associations between intraoperative F2-isoprostanes and isofurans and delirium (primary outcome) and postoperative ubiquitin carboxyl-terminal hydrolase isozyme L1 (secondary outcome), and we assessed if S100 calcium-binding protein B modified these associations.
Results: Delirium occurred in 109 of 400 (27.3%) patients for a median (10th, 90th percentile) of 1.0 (0.5, 3.0) days. In the total cohort, plasma ubiquitin carboxyl-terminal hydrolase isozyme L1 concentration was 6.3 ng/ml (2.7, 14.9) at baseline and 12.4 ng/ml (7.9, 31.2) on postoperative day 1. F2-isoprostanes and isofurans increased throughout surgery, and the log-transformed sum of intraoperative F2-isoprostanes and isofurans was independently associated with increased odds of postoperative delirium (odds ratio, 3.70 [95% CI, 1.41 to 9.70]; P = 0.008) and with increased postoperative ubiquitin carboxyl-terminal hydrolase isozyme L1 (ratio of geometric means, 1.42 [1.11 to 1.81]; P = 0.005). The association between increased intraoperative F2-isoprostanes and isofurans and increased postoperative ubiquitin carboxyl-terminal hydrolase isozyme L1 was amplified in patients with elevated S100 calcium-binding protein B (P = 0.049).
Conclusions: Intraoperative oxidative damage was associated with increased postoperative delirium and neuronal injury, and the association between oxidative damage and neuronal injury was stronger among patients with increased blood-brain barrier disruption.
Conflict of interest statement
Figures
Comment in
-
Oxidative Stress Response and Delirium after Cardiac Surgery: Can Circulating Biomarkers Refine New Therapeutic Paradigms?Anesthesiology. 2020 Mar;132(3):418-420. doi: 10.1097/ALN.0000000000003097. Anesthesiology. 2020. PMID: 31929329 No abstract available.
References
-
- Evered L, Silbert B, Knopman DS, Scott DA, DeKosky ST, Rasmussen LS, Oh ES, Crosby G, Berger M, Eckenhoff RG, Nomenclature Consensus Working Group: Recommendations for the Nomenclature of Cognitive Change Associated with Anaesthesia and Surgery-2018. Anesthesiology 2018; 129: 872–879 - PubMed
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr., Inouye SK, Bernard GR, Dittus RS Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004; 291: 1753–62 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
