

Pancreas lipiodol embolism induced acute necrotizing pancreatitis following transcatheter arterial chemoembolization for hepatocellular carcinoma: A case report and literature review
- PMID: 31770228
- PMCID: PMC6890338
- DOI: 10.1097/MD.0000000000018095
Pancreas lipiodol embolism induced acute necrotizing pancreatitis following transcatheter arterial chemoembolization for hepatocellular carcinoma: A case report and literature review
Abstract
Rationale: Transcatheter arterial chemoembolization (TACE) is recognized as one of the most commonly used modalities for non-surgical treatment for advanced hepatocellular carcinoma (HCC). Ectopic lipiodol embolism is an extremely rare complication of TACE.
Patient concerns: A 61-year-old man who had a 10-year history of cirrhosis caused by hepatitis B infection was diagnosed with ascites and HCC. Subsequently, the patient underwent TACE. However, he experienced persistent left upper abdominal pain, poor appetite, nausea, moderate fever and accompanied by elevation of serum and urine amylase on the 2nd and 3nd day after treatment.
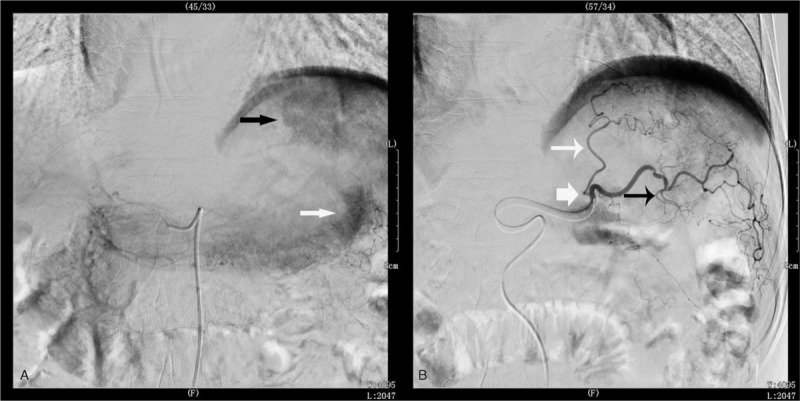
Diagnoses: The patient was diagnosed as having acute hemorrhagic necrotizing pancreatitis based on biochemical and inflammatory markers and CT findings. We deduced that the acute necrotizing pancreatitis was caused by a small branch of the left hepatic artery feeding the pancreas tail and embolizing the drug and lipiodol shunting to the tail of the pancreas.
Interventions: The patient was treated for 5 days according to the comprehensive treatment of acute necrotizing pancreatitis, by the inhibition of the secretion of pancreatic juice, relieving pain, and total parenteral nutrition and forbidding diet. The symptoms of the patient were observed to improve, and SAMS and urinary amylase (UAMS) level decreased to 143 IU/L and 254 IU/L, respectively and oral diet was permitted.
Outcome: After a period of 2 weeks, the contrast abdominal CT showed slightly decreased fluid collection of the peri-pancreatic space. Moreover, it also showed flocculous and linear high-density shadow in the pancreatic tail, suggesting lipiodol deposition in the pancreatic tail. Subsequently, the symptoms were observed to abate, and the patient left the hospital. On the 21st day after TACE, the patient had a follow up in our outpatient department; the biochemical characteristics and inflammatory markers were observed to be normal CONCLUSION:: AP is still a rare complication after TACE. Etiology is still attributed to the occurrence of shunting and embolization drug reflux. Strategies strengthening the catheter tip that is placed as close to the distal branches of the hepatic artery for the possible careful injection of embolic materials is still the key to avoid post-TACE AP.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Wang Z, Li Z, Ji Y. Postoperative transcatheter arterial chemoembolization should be recommended in the hepatocellular carcinoma treatment guidelines of the American Association for the Study of Liver Diseases. Hepatology 2011;54:1489–90. - PubMed
-
- Piscaglia F, Tovoli F, Pini P, et al. A new horizon in the prevention of the postembolization syndrome after transcatheter arterial chemoembolization for hepatocellular carcinoma. Hepatology 2018;67:467–9. - PubMed
-
- Nie Q, Wu H, Guo P, et al. Cerebral lipiodol embolism following abdomen trauma in a patient with hepatocellular carcinoma treated with transcatheter arterial chemoembolization. Acta Neurolog Belgica 2015;115:459–61. - PubMed
-
- Li Z, Ni RF, Busireddy KK, et al. Cerebral lipiodol embolism following transcatheter arterial chemoembolization for hepatocellular carcinoma: a report of two cases and literature review. Chin Med J 2011;124:4355–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
