

Neuropathologic Correlates of White Matter Hyperintensities in a Community-Based Cohort of Older Adults
- PMID: 31771057
- PMCID: PMC6996196
- DOI: 10.3233/JAD-190687
Neuropathologic Correlates of White Matter Hyperintensities in a Community-Based Cohort of Older Adults
Abstract
Background: The association of white matter hyperintensities (WMH) with age-related vascular and neurodegenerative pathologies remains incompletely understood.
Objective: The objective of this work was to elucidate the neuropathologic correlates of WMH in a large community-based cohort of older adults.
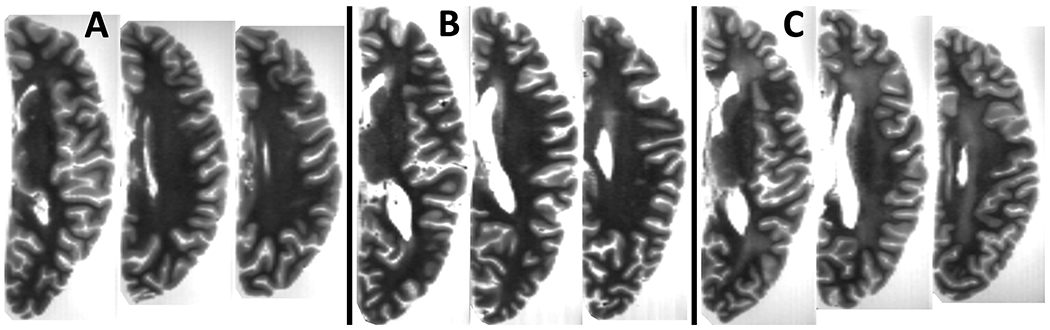
Methods: Cerebral hemispheres from 603 community-based older adults were imaged with MRI ex vivo. All participants underwent annual clinical evaluation, cognitive assessment, and neuropathologic examination. WMH burden was assessed using a modified Fazekas rating scale. Multiple ordinal logistic regression was used to test the association of WMH burden with an array of age-related neuropathologies, adjusting for demographics. Mixed effects models of cognition controlling for neuropathologies and demographics were used to determine whether WMH burden contributes to cognitive decline beyond measured pathologies.
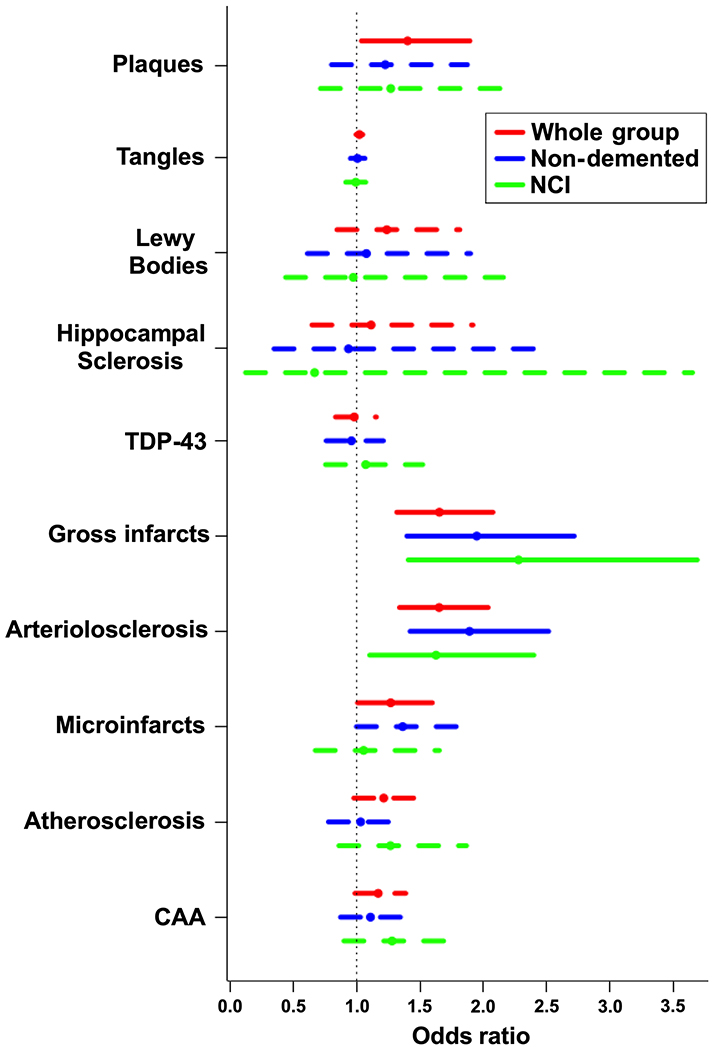
Results: WMH burden in the whole group was associated with both vascular and Alzheimer's disease (AD) pathologies: arteriolosclerosis (p < 10-4), gross (p < 10-4), and microscopic infarcts (p = 0.04), and amyloid-β plaques (p = 0.028). In non-demented participants (mild or no cognitive impairment) (N = 332), WMH burden was related to gross infarcts (p = 10-4) and arteriolosclerosis (p < 10-4), but not to AD pathology. Similarly, in those with no cognitive impairment (N = 178), WMH burden was related to gross infarcts (p = 8×10-4) and arteriolosclerosis (p = 0.014). WMH burden was associated with faster decline in perceptual speed in both the whole (p = 0.038) and non-demented (p = 0.006) groups.
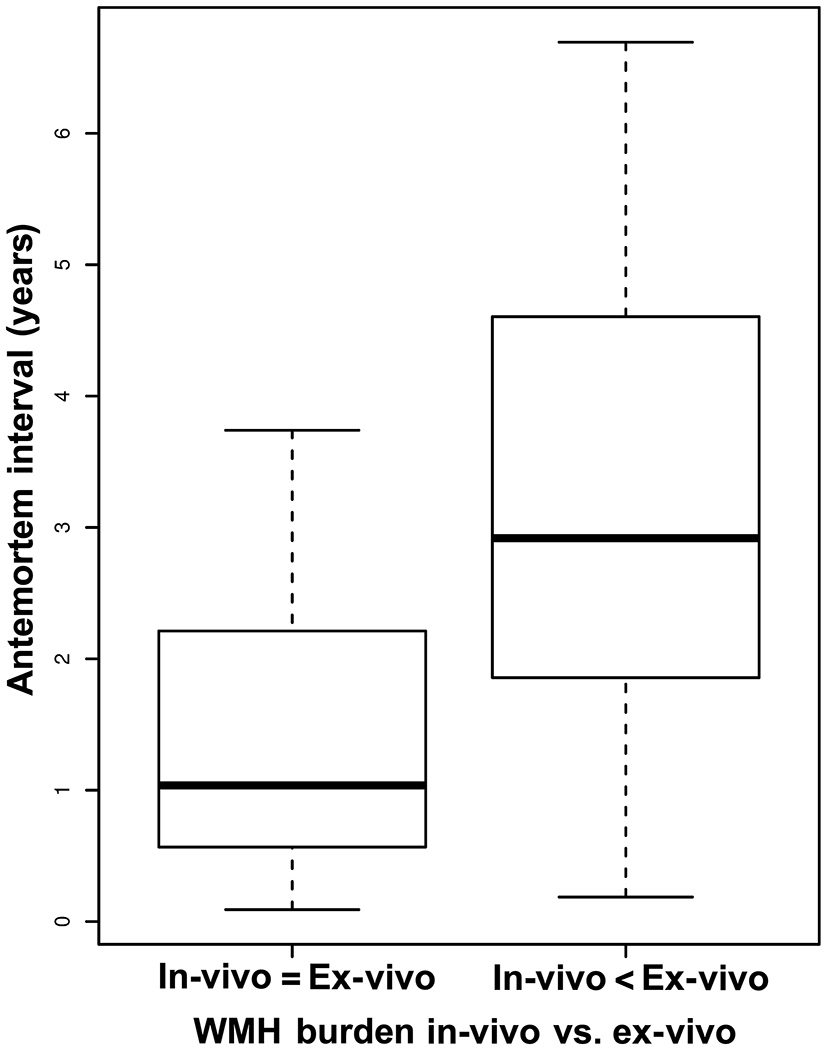
Conclusion: WMH burden has independent associations with vascular pathologies in older adults regardless of clinical status, and with AD pathology later in the progression of AD. Moreover, WMH burden may reflect additional tissue injury not captured with traditional neuropathologic indices.
Keywords: Cognition; magnetic resonance imaging; pathology; white matter hyperintensities.
Conflict of interest statement
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Figures
References
-
- de Leeuw FE, de Groot JC, Achten E, Oudkerk M, Ramos LM, Heijboer R, Hofman A, Jolles J, van Gijn J, Breteler MM (2001) Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study. J. Neurol. Neurosurg. Psychiatry 70, 9–14. - PMC - PubMed
-
- DeCarli C, Massaro J, Harvey D, Hald J, Tullberg M, Au R, Beiser A, D’Agostino R, Wolf PA (2005) Measures of brain morphology and infarction in the framingham heart study: establishing what is normal. Neurobiol. Aging 26, 491–510. - PubMed
-
- Habes M, Sotiras A, Erus G, Toledo JB, Janowitz D, Wolk DA, Shou H, Bryan NR, Doshi J, Völzke H, Schminke U, Hoffmann W, Resnick SM, Grabe HJ, Davatzikos C (2018) White matter lesions: Spatial heterogeneity, links to risk factors, cognition, genetics, and atrophy. Neurology 91, e964–e975. - PMC - PubMed
-
- Dufouil C, Chalmers J, Coskun O, Besançon V, Bousser M-G, Guillon P, MacMahon S, Mazoyer B, Neal B, Woodward M, Tzourio-Mazoyer N, Tzourio C, PROGRESS MRI Substudy Investigators (2005) Effects of Blood Pressure Lowering on Cerebral White Matter Hyperintensities in Patients With Stroke. Circulation 112, 1644–1650. - PubMed
Publication types
MeSH terms
Grants and funding
- UH3 NS100599/NS/NINDS NIH HHS/United States
- TL1 TR002375/TR/NCATS NIH HHS/United States
- R01 AG017917/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- R01 AG022018/AG/NIA NIH HHS/United States
- R01 AG034374/AG/NIA NIH HHS/United States
- UF1 NS100599/NS/NINDS NIH HHS/United States
- R01 AG056405/AG/NIA NIH HHS/United States
- UM1 MH130981/MH/NIMH NIH HHS/United States
- R01 AG042210/AG/NIA NIH HHS/United States
- UH2 NS100599/NS/NINDS NIH HHS/United States
- R01 AG064233/AG/NIA NIH HHS/United States
- RF1 AG022018/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
