

Intra-operative optical coherence tomography in glaucoma surgery-a systematic review
- PMID: 31772380
- PMCID: PMC7002696
- DOI: 10.1038/s41433-019-0689-3
Intra-operative optical coherence tomography in glaucoma surgery-a systematic review
Abstract
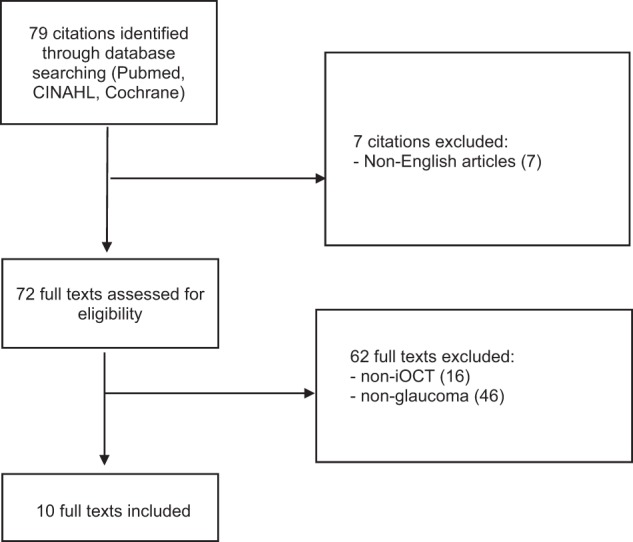
The application of the OCT in clinical ophthalmology has expanded significantly since its introduction more than 20 years ago. There has been recent growing interest in the application of intra-operative optical coherence tomography (iOCT). The iOCT's ability to enhance visualisation and depth appreciation has the potential to be further exploited in glaucoma surgery, especially with the emergence of Minimally Invasive Glaucoma Surgery (MIGS)-to facilitate targeted device placement and fine surgical manoeuvres in the angles, the sub-conjunctival layer and the suprachoroidal space. Hence, this study aims to appraise the current literature on the applications of iOCT in glaucoma surgery. A total of 79 studies were identified following a literature search adhering to PRISMA guidelines. After full text evaluation, 10 studies discussing iOCT use in glaucoma surgery were included. Traditional glaucoma filtering procedures reviewed included trabeculectomy surgery, goniosynechiolysis, bleb needling and glaucoma drainage device implantation. MIGS procedures reviewed included canaloplasty, trabecular aspiration, ab-interno trabectome and the XEN45 gel stent. iOCT use in ophthalmic surgery is becoming increasingly prevalent and has already been applied in various surgeries and procedures in the field of glaucoma. With the greater adoption of MIGS, iOCT may further contribute in facilitating surgical techniques and improving outcomes. While iOCT offers many advantages, there are still limitations to be overcome-iOCT technology continues to evolve to optimise imaging quality and user-experience.
摘要: 自20年前OCT投入眼科临床应用至今, 其应用范围不断扩展。近期术中应用光学相干断层扫描 (iOCT) 的热度不断攀升, iOCT能够提升可视化程度和深层组织的鉴别能力, 有助于其在青光眼手术中的进一步拓展应用, 尤其在青光眼微创手术(MIGS)中——它有助于在房角、结膜下和脉络膜上腔进行有针对性的引流装置的放置与精细的手术操作。本文旨在评价目前已发表的在青光眼术中应用iOCT的文献。根据PRISMA指南的文献检索标准共选出79篇研究, 经过全文评估后, 录入10篇讨论青光眼术中应用iOCT的文献。关于传统青光眼滤过术的文献包括小梁切除术、房角粘连松解术、滤过泡穿刺术和青光眼引流装置。关于MIGS手术的文献包括Schlemm氏管成形术、小梁吸除术、小梁消融术和XEN凝胶引流支架引流装置植入术。iOCT在眼科手术中的应用越来越普遍, 并且已经在青光眼领域的各类手术中使用。iOCT在MIGS中的积极应用会改进手术技术并改善手术疗效。尽管iOCT有很多优点, 但仍有需要克服的问题——iOCT技术需要继续提升以及优化成像质量和用户的体验。.
Conflict of interest statement
BCHA has previously received funding from Glaukos Corporation (travel, research), Santen Pharmaceutical Co., Ltd. (travel, consultant) and Allergan plc (travel, research, consultant). He has not received funding for his work in this publication. SD has consulted for New World Medical and received funding (travel, research). He has not received funding for his work in this publication. The remaining author declares that he has no conflict of interest.
Figures
References
-
- Swanson EA, Huang D. Ophthalmic OCT reaches $1 billion per year. Retinal Physician. 2011;53:58–9.
-
- Eguchi H, Kusaka S, Arimura-Koike E, Tachibana K, Tsujioka D, Fukuda M, et al. Intraoperative optical coherence tomography (RESCAN® 700) for detecting iris incarceration and iridocorneal adhesion during keratoplasty. Int Ophthalmol. 2017;37:761–5. - PubMed
-
- Saad A, Guilbert E, Grise-Dulac A, Sabatier P, Gatinel D. Intraoperative OCT-assisted DMEK: 14 consecutive cases. Cornea. 2015;34:802–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
