Intraoperative hypotension and its prediction
- PMID: 31772395
- PMCID: PMC6868662
- DOI: 10.4103/ija.IJA_624_19
Intraoperative hypotension and its prediction
Abstract
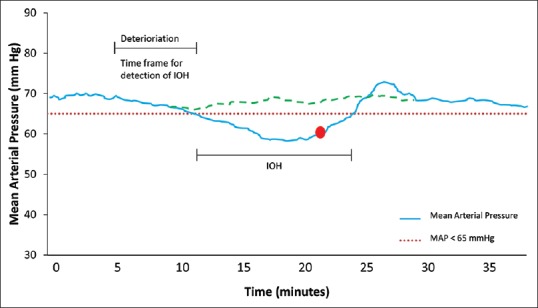
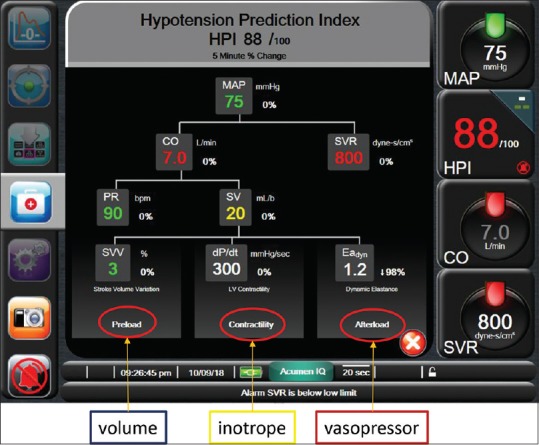
Intraoperative hypotension (IOH) very commonly accompanies general anaesthesia in patients undergoing major surgical procedures. The development of IOH is unwanted, since it is associated with adverse outcomes such as acute kidney injury and myocardial injury, stroke and mortality. Although the definition of IOH is variable, harm starts to occur below a mean arterial pressure (MAP) threshold of 65 mmHg. The odds of adverse outcome increase for increasing duration and/or magnitude of IOH below this threshold, and even short periods of IOH seem to be associated with adverse outcomes. Therefore, reducing the hypotensive burden by predicting and preventing IOH through proactive appropriate treatment may potentially improve patient outcome. In this review article, we summarise the current state of the prediction of IOH by the use of so-called machine-learning algorithms. Machine-learning algorithms that use high-fidelity data from the arterial pressure waveform, may be used to reveal 'traits' that are unseen by the human eye and are associated with the later development of IOH. These algorithms can use large datasets for 'training', and can subsequently be used by clinicians for haemodynamic monitoring and guiding therapy. A first clinically available application, the hypotension prediction index (HPI), is aimed to predict an impending hypotensive event, and additionally, to guide appropriate treatment by calculated secondary variables to asses preload (dynamic preload variables), contractility (dP/dtmax), and afterload (dynamic arterial elastance, Eadyn). In this narrative review, we summarise the current state of the prediction of hypotension using such novel, automated algorithms and we will highlight HPI and the secondary variables provided to identify the probable origin of the (impending) hypotensive event.
Keywords: Blood pressure; hemodynamic monitoring; hypotension prediction index; machine learning; predictive analysis.
Copyright: © 2019 Indian Journal of Anaesthesia.
Conflict of interest statement
TWLS received research grants and honoraria from Edwards Lifesciences (Irvine, CA, USA) and Masimo Inc. (Irvine, CA, USA) for consulting and lecturing and from Pulsion Medical Systems SE (Feldkirchen, Germany) for lecturing.
Figures
References
-
- Wesselink EM, Kappen TH, Torn HM, Slooter AJ, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br J Anaesth. 2018;121:706–21. - PubMed
-
- Maheshwari K, Turan A, Mao G, Yang D, Niazi AK, Agarwal D, et al. The association of hypotension during non-cardiac surgery, before and after skin incision, with postoperative acute kidney injury: A retrospective cohort analysis. Anaesthesia. 2018;73:1223–8. - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: Toward an empirical definition of hypotension. Anesthesiology. 2013;119:507–15. - PubMed
-
- Salmasi V, Maheshwari K, Yang D, Mascha EJ, Singh A, Sessler DI, et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Anesthesiology. 2017;126:47–65. - PubMed
-
- Sun LY, Wijeysundera DN, Tait GA, Beattie WS. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology. 2015;123:515–23. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical