

Mindfulness-Based Blood Pressure Reduction (MB-BP): Stage 1 single-arm clinical trial
- PMID: 31774807
- PMCID: PMC6881004
- DOI: 10.1371/journal.pone.0223095
Mindfulness-Based Blood Pressure Reduction (MB-BP): Stage 1 single-arm clinical trial
Abstract
Background and objectives: Impacts of mindfulness-based programs on blood pressure remain equivocal, possibly because the programs are not adapted to engage with determinants of hypertension, or due to floor effects. Primary objectives were to create a customized Mindfulness-Based Blood Pressure Reduction (MB-BP) program, and to evaluate acceptability, feasibility, and effects on hypothesized proximal self-regulation mechanisms. Secondary outcomes included modifiable determinants of blood pressure (BP), and clinic-assessed systolic blood pressure (SBP).
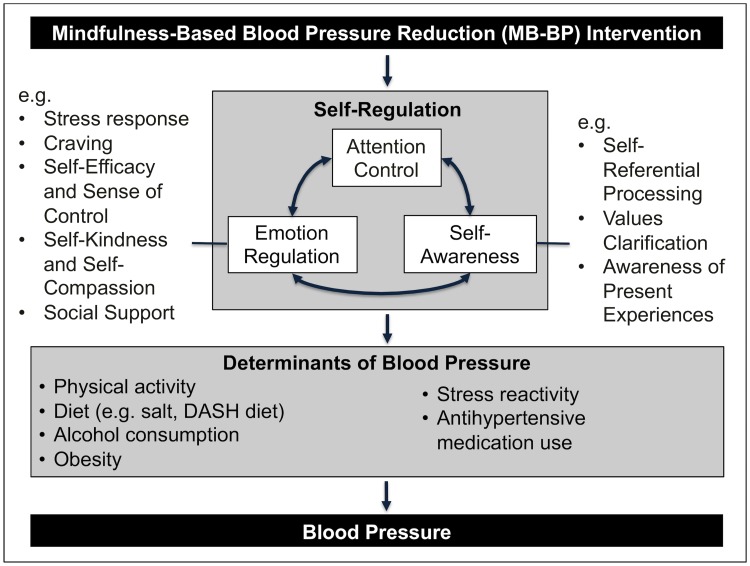
Methods: This was a Stage 1 single-arm trial with one year follow-up. Focus groups and in-depth interviews were performed to evaluate acceptability and feasibility. Self-regulation outcomes, and determinants of BP, were assessed using validated questionnaires or objective assessments. The MB-BP curriculum was adapted from Mindfulness-Based Stress Reduction to direct participants' mindfulness skills towards modifiable determinants of blood pressure.
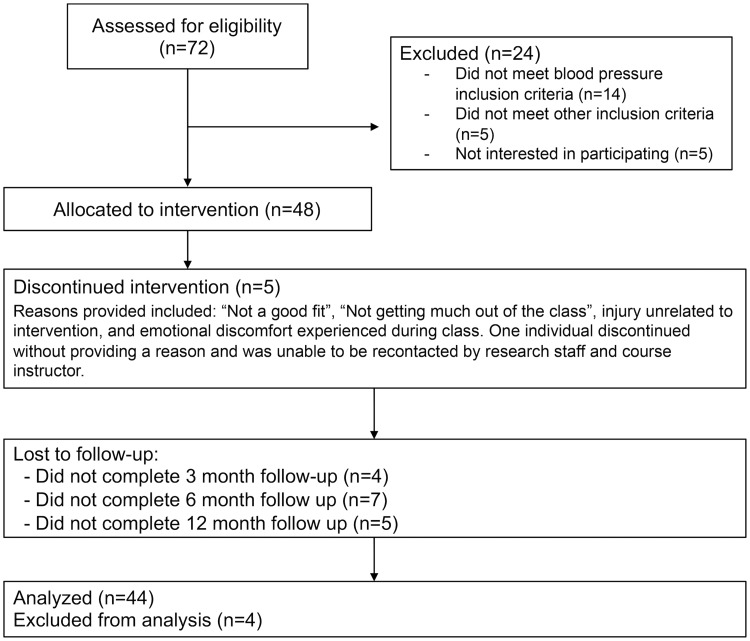
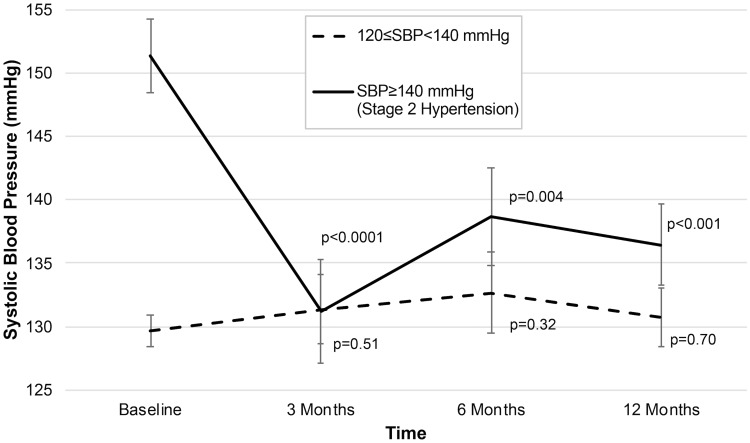
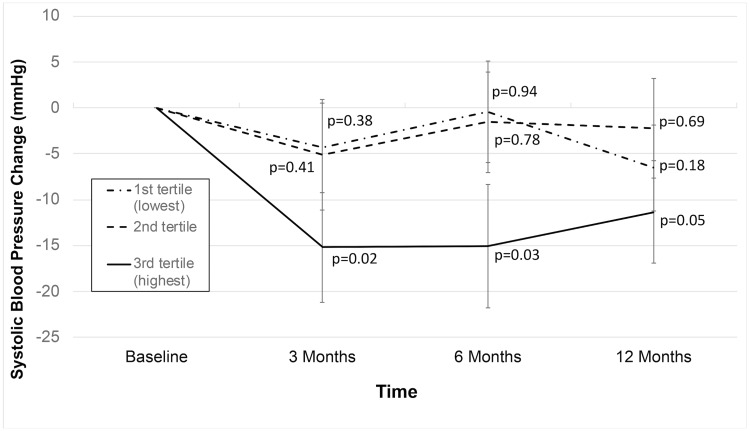
Results: Acceptability and feasibility findings showed that of 53 eligible participants, 48 enrolled (91%). Of these, 43 (90%) attended at least 7 of the 10 MB-BP classes; 43 were followed to one year (90%). Focus groups (n = 19) and semi-structured interviews (n = 10) showed all participants viewed the delivery modality favorably, and identified logistic considerations concerning program access as barriers. A priori selected primary self-regulation outcomes showed improvements at one-year follow-up vs. baseline, including attention control (Sustained Attention to Response Task correct no-go score, p<0.001), emotion regulation (Difficulties in Emotion Regulation Score, p = 0.02), and self-awareness (Multidimensional Assessment of Interoceptive Awareness, p<0.001). Several determinants of hypertension were improved in participants not adhering to American Heart Association guidelines at baseline, including physical activity (p = 0.02), Dietary Approaches to Stop Hypertension-consistent diet (p<0.001), and alcohol consumption (p<0.001). Findings demonstrated mean 6.1 mmHg reduction in SBP (p = 0.008) at one year follow-up; effects were most pronounced in Stage 2 uncontrolled hypertensives (SBP≥140 mmHg), showing 15.1 mmHg reduction (p<0.001).
Conclusion: MB-BP has good acceptability and feasibility, and may engage with self-regulation and behavioral determinants of hypertension.
Conflict of interest statement
Dr. Loucks is Director of the Mindfulness Center at Brown University. The Mindfulness Center, a non-profit entity, has an Education Unit that provides mindfulness based program delivery to the general public for fees. However, Dr. Loucks’s salary is not tied to quantity or content of programs offered through the Mindfulness Center. Dr. Loucks is a practicing Buddhist, and while the mindfulness elements of MBSR and MB-BP have roots in Buddhist philosophy, the intervention is designed for use in secular health settings, and does not encourage any particular religion. Additionally, conditions were put in place to limit the potential bias of Dr. Loucks’s religious affiliation on study data interpretation. For example, the primary outcomes were preregistered on ClinicalTrials.gov. Dr. Loucks did not have access to the data file. He also did not perform the statistical analyses which were performed by an independent data analyst (Y.L.), or the qualitative coding and analyses that were led by three trained co-authors (W.N., A.W., J.W.). The data have been made publicly available using the OpenScience Framework. Dr. Britton is an MBSR and Mindfulness-Based Cognitive Therapy teacher. She has received payment to provide trainings on best practices for harms monitoring, measurement, and management. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2017. Epub 2017/11/15. 10.1161/HYP.0000000000000066 . - DOI - PubMed
-
- Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016;134(6):441–50. Epub 2016/08/10. 10.1161/CIRCULATIONAHA.115.018912 . - DOI - PMC - PubMed
-
- World Health Report 2002. Reducing risks, promoting healthy life. World Health Organization. Geneva, Switzerland. http://wwwwhoint/whr/2002. 2002. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
