

Mortality risk over time after early fluid resuscitation in African children
- PMID: 31775837
- PMCID: PMC6882199
- DOI: 10.1186/s13054-019-2619-y
Mortality risk over time after early fluid resuscitation in African children
Abstract
Background: African children hospitalised with severe febrile illness have a high risk of mortality. The Fluid Expansion As Supportive Therapy (FEAST) trial (ISCRTN 69856593) demonstrated increased mortality risk associated with fluid boluses, but the temporal relationship to bolus therapy and underlying mechanism remains unclear.
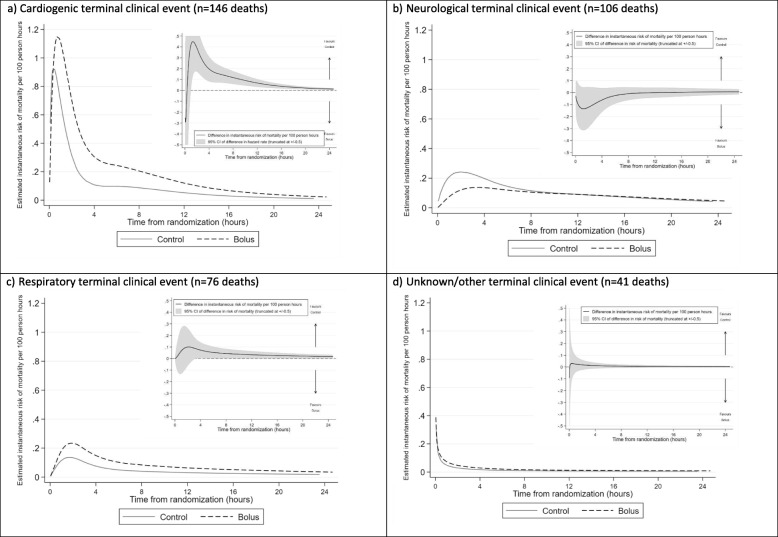
Methods: In a post hoc retrospective analysis, flexible parametric models were used to compare change in mortality risk post-randomisation in children allocated to bolus therapy with 20-40 ml/kg 5% albumin or 0.9% saline over 1-2 h or no bolus (control, 4 ml/kg/hour maintenance), overall and for different terminal clinical events (cardiogenic, neurological, respiratory, or unknown/other).
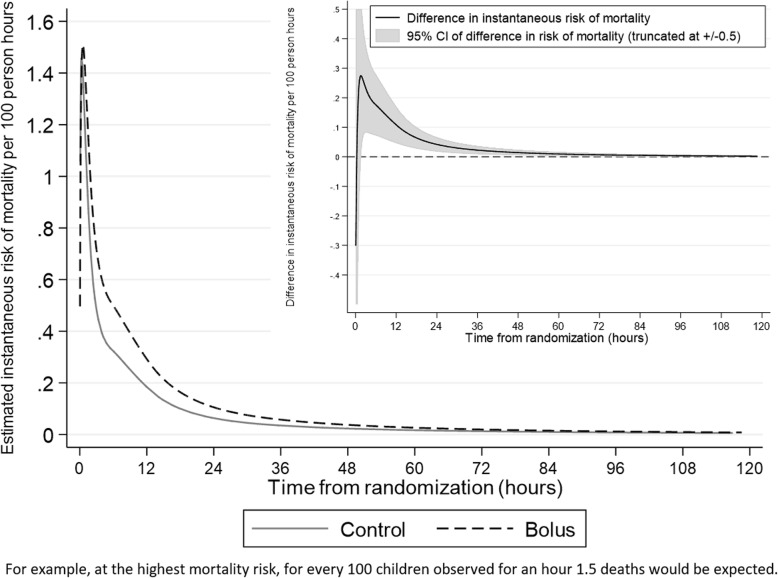
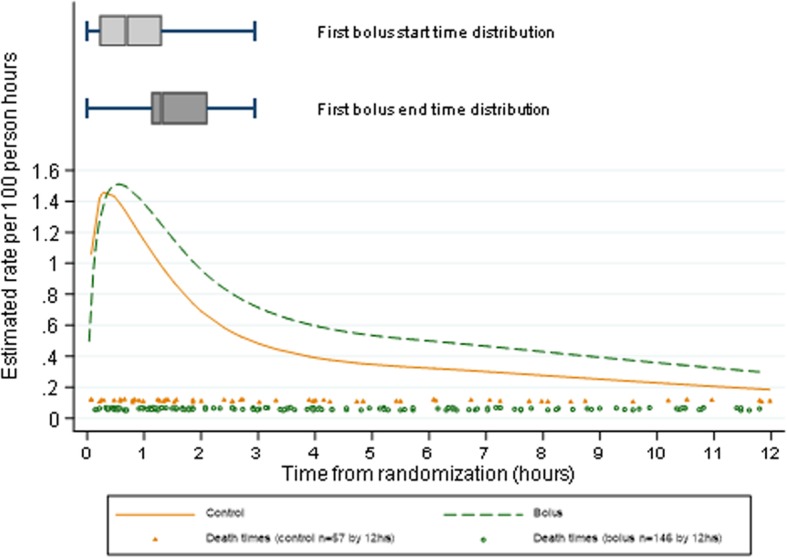
Results: Two thousand ninety-seven and 1041 children were randomised to bolus vs no bolus, of whom 254 (12%) and 91 (9%) respectively died within 28 days. Median (IQR) bolus fluid in the bolus groups received by 4 h was 20 (20, 40) ml/kg and was the same at 8 h; total fluids received in bolus groups at 4 h and 8 h were 38 (28, 43) ml/kg and 40 (30, 50) ml/kg, respectively. Total fluid volumes received in the control group by 4 h and 8 h were median (IQR) 10 (6, 15) ml/kg and 10 (10, 26) ml/kg, respectively. Mortality risk was greatest 30 min post-randomisation in both groups, declining sharply to 4 h and then more slowly to 28 days. Maximum mortality risk was similar in bolus and no bolus groups; however, the risk declined more slowly in the bolus group, with significantly higher mortality risk compared to the no bolus group from 1.6 to 101 h (4 days) post-randomisation. The delay in decline in mortality risk in the bolus groups was most pronounced for cardiogenic modes of death.
Conclusions: The increased risk from bolus therapy was not due to a mechanism occurring immediately after bolus administration. Excess mortality risk in the bolus group resulted from slower decrease in mortality risk over the ensuing 4 days. Thus, administration of modest bolus volumes appeared to prevent mortality risk declining at the same rate that it would have done without a bolus, rather than harm associated with bolus resulting from a concurrent increased risk of death peri-bolus administration.
Trial registration: ISRCTN69856593. Date of registration 15 December 2008.
Keywords: Africa; Fluid resuscitation; Mortality risk; Paediatric shock; Parametric models.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment on
-
Mortality after fluid bolus in African children with severe infection.N Engl J Med. 2011 Jun 30;364(26):2483-95. doi: 10.1056/NEJMoa1101549. Epub 2011 May 26. N Engl J Med. 2011. PMID: 21615299 Clinical Trial.
References
-
- Lambert PC, Royston P. Further development of flexible parametric models for survival analysis. Stata J. 2009;9(2):265–290. doi: 10.1177/1536867X0900900206. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
