

Short term exposure to fine particulate matter and hospital admission risks and costs in the Medicare population: time stratified, case crossover study
- PMID: 31776122
- PMCID: PMC6880251
- DOI: 10.1136/bmj.l6258
Short term exposure to fine particulate matter and hospital admission risks and costs in the Medicare population: time stratified, case crossover study
Abstract
Objective: To assess risks and costs of hospital admission associated with short term exposure to fine particulate matter with diameter less than 2.5 µm (PM2.5) for 214 mutually exclusive disease groups.
Design: Time stratified, case crossover analyses with conditional logistic regressions adjusted for non-linear confounding effects of meteorological variables.
Setting: Medicare inpatient hospital claims in the United States, 2000-12 (n=95 277 169).
Participants: All Medicare fee-for-service beneficiaries aged 65 or older admitted to hospital.
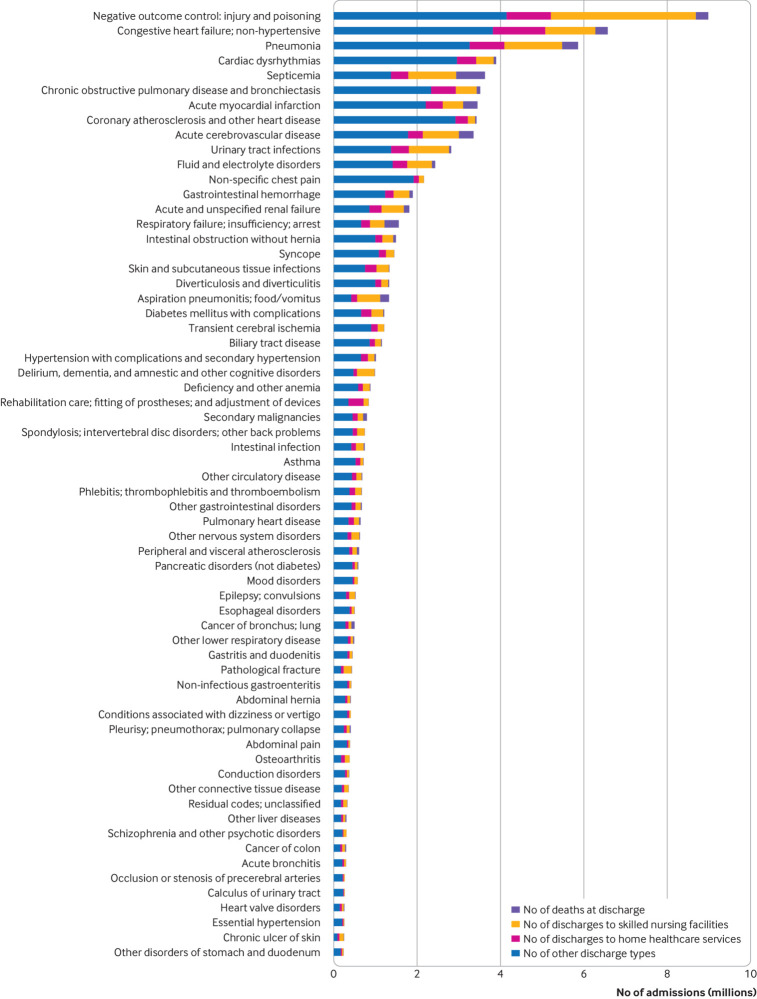
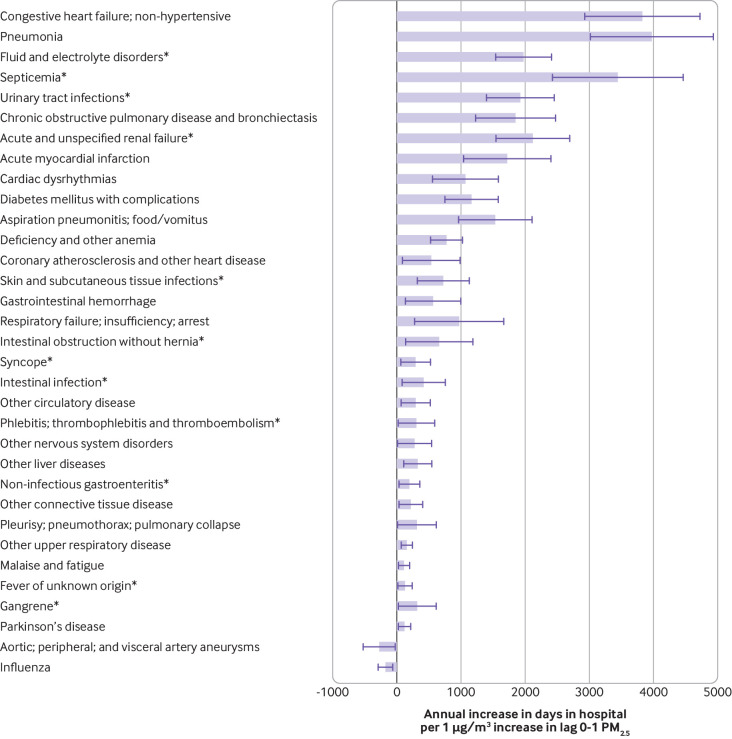
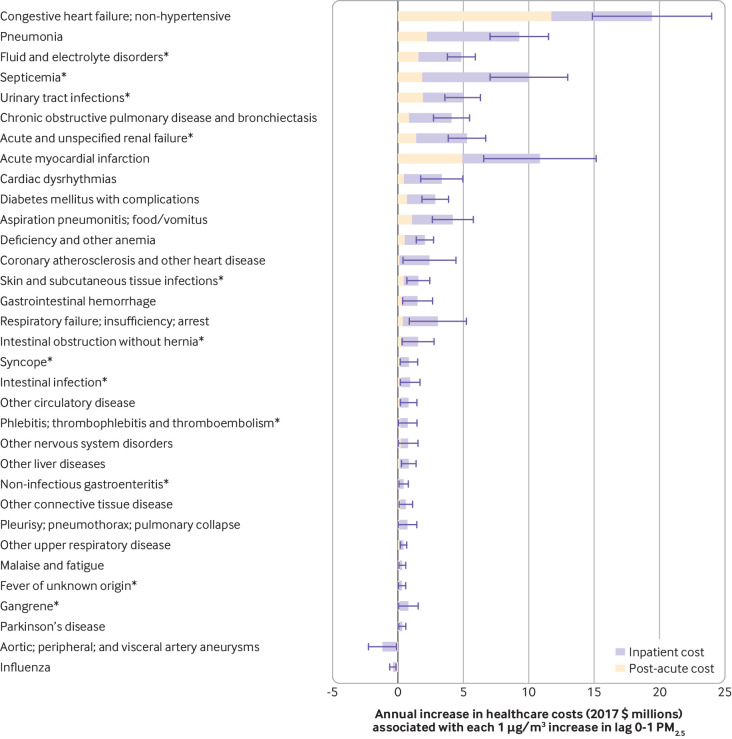
Main outcome measures: Risk of hospital admission, number of admissions, days in hospital, inpatient and post-acute care costs, and value of statistical life (that is, the economic value used to measure the cost of avoiding a death) due to the lives lost at discharge for 214 disease groups.
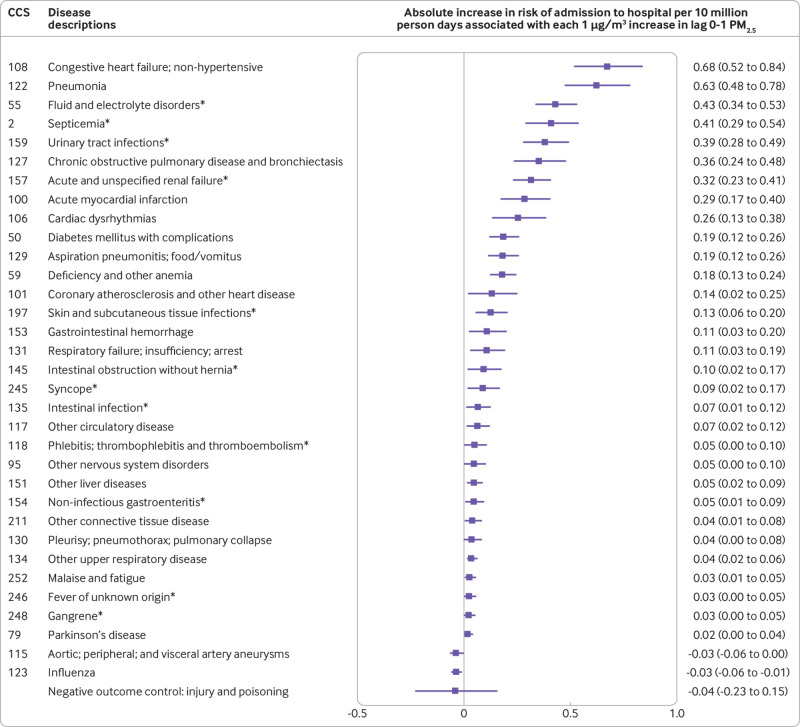
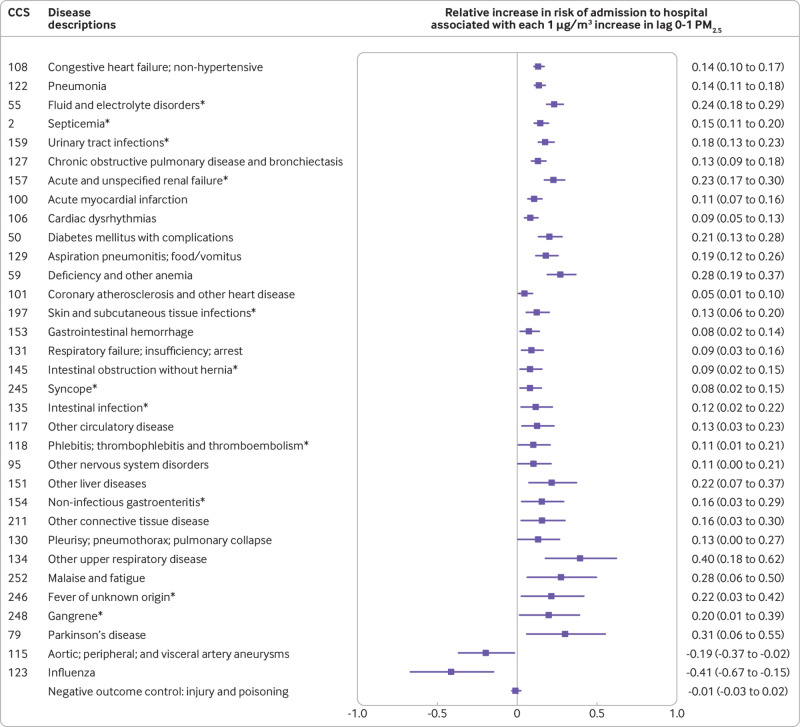
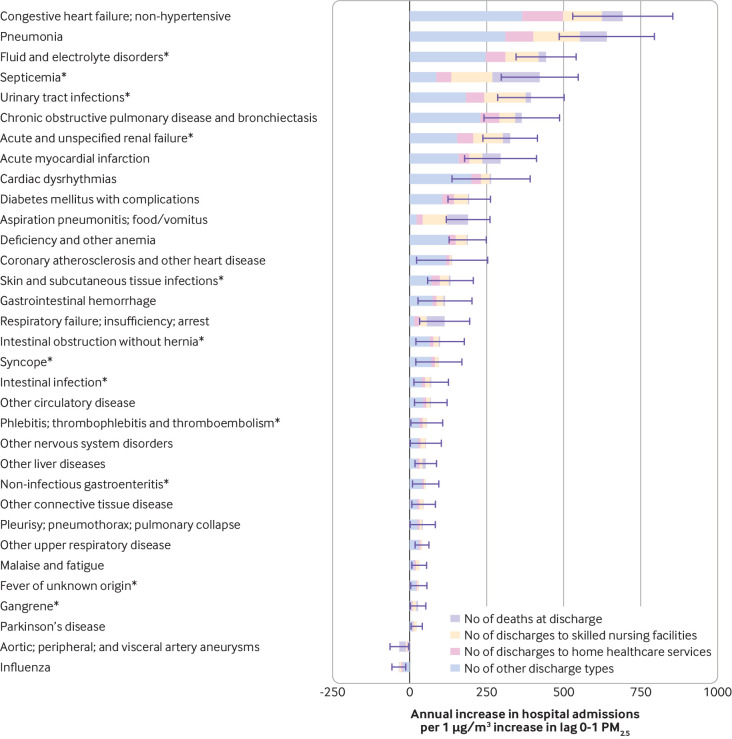
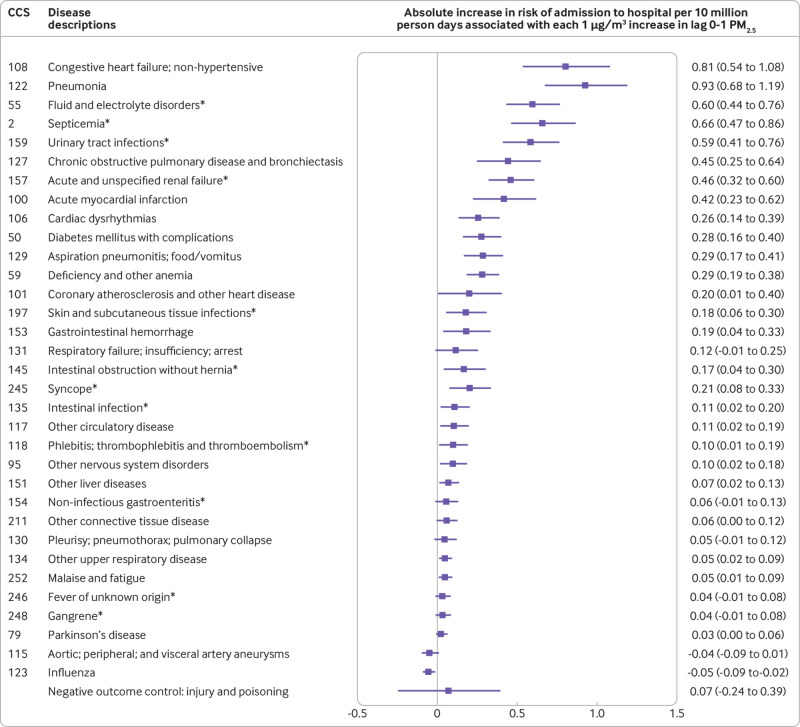
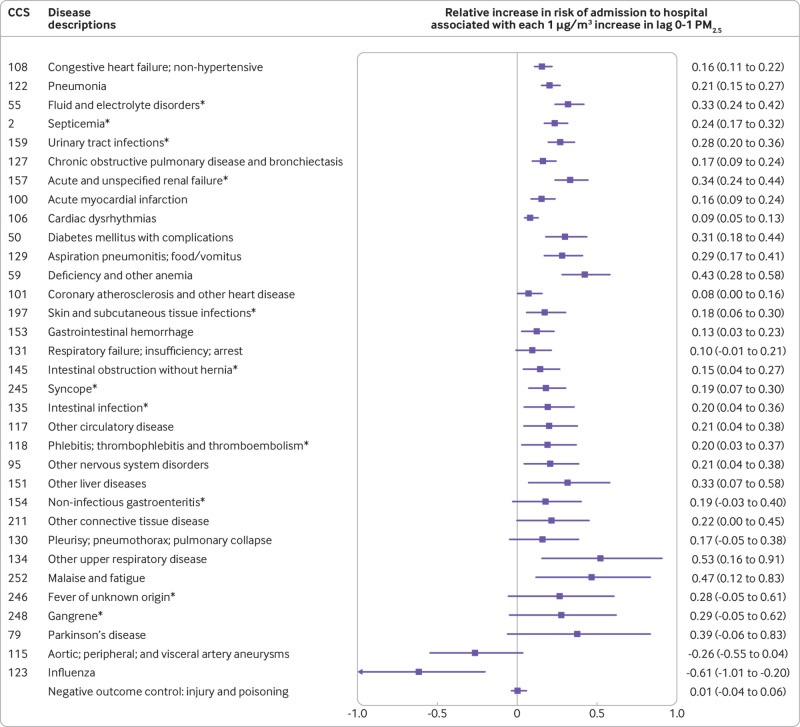
Results: Positive associations between short term exposure to PM2.5 and risk of hospital admission were found for several prevalent but rarely studied diseases, such as septicemia, fluid and electrolyte disorders, and acute and unspecified renal failure. Positive associations were also found between risk of hospital admission and cardiovascular and respiratory diseases, Parkinson's disease, diabetes, phlebitis, thrombophlebitis, and thromboembolism, confirming previously published results. These associations remained consistent when restricted to days with a daily PM2.5 concentration below the WHO air quality guideline for the 24 hour average exposure to PM2.5. For the rarely studied diseases, each 1 µg/m3 increase in short term PM2.5 was associated with an annual increase of 2050 hospital admissions (95% confidence interval 1914 to 2187 admissions), 12 216 days in hospital (11 358 to 13 075), US$31m (£24m, €28m; $29m to $34m) in inpatient and post-acute care costs, and $2.5bn ($2.0bn to $2.9bn) in value of statistical life. For diseases with a previously known association, each 1 µg/m3 increase in short term exposure to PM2.5 was associated with an annual increase of 3642 hospital admissions (3434 to 3851), 20 098 days in hospital (18 950 to 21 247), $69m ($65m to $73m) in inpatient and post-acute care costs, and $4.1bn ($3.5bn to $4.7bn) in value of statistical life.
Conclusions: New causes and previously identified causes of hospital admission associated with short term exposure to PM2.5 were found. These associations remained even at a daily PM2.5 concentration below the WHO 24 hour guideline. Substantial economic costs were linked to a small increase in short term PM2.5.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the NIH, NIH/NCI, HEI, and US EPA for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
The health effects of fine particulate air pollution.BMJ. 2019 Nov 27;367:l6609. doi: 10.1136/bmj.l6609. BMJ. 2019. PMID: 31776108 No abstract available.
References
-
- Brook RD, Franklin B, Cascio W, et al. Expert Panel on Population and Prevention Science of the American Heart Association Air pollution and cardiovascular disease: a statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004;109:2655-71. 10.1161/01.CIR.0000128587.30041.C8 - DOI - PubMed
-
- Air quality guidelines WHO. Geneva: World Health Organization. 2006.
-
- World Health Organization (WHO) WHO expert consultation: available evidence for the future update of the WHO global air quality guidelines (AQGs). WHO, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical