

Outcome and prognostic factors of Pneumocystis jirovecii pneumonia in immunocompromised adults: a prospective observational study
- PMID: 31776705
- PMCID: PMC6881486
- DOI: 10.1186/s13613-019-0604-x
Outcome and prognostic factors of Pneumocystis jirovecii pneumonia in immunocompromised adults: a prospective observational study
Abstract
Background: Pneumocystis jirovecii pneumonia (PJP) remains a severe disease associated with high rates of invasive mechanical ventilation (MV) and mortality. The objectives of this study were to assess early risk factors for severe PJP and 90-day mortality, including the broncho-alveolar lavage fluid cytology profiles at diagnosis.
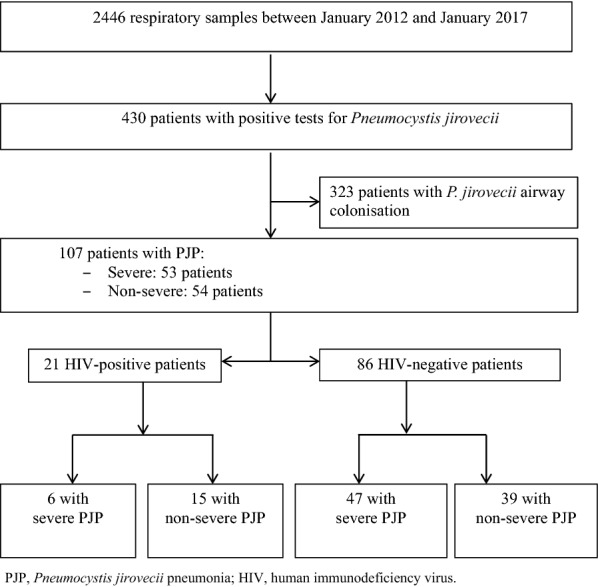
Methods: We prospectively enrolled all patients meeting pre-defined diagnostic criteria for PJP admitted at Nantes university hospital, France, from January 2012 to January 2017. Diagnostic criteria for PJP were typical clinical features with microbiological confirmation of P. jirovecii cysts by direct examination or a positive specific quantitative real-time polymerase chain reaction (PCR) assay. Severe PJP was defined as hypoxemic acute respiratory failure requiring high-flow nasal oxygen with at least 50% FiO2, non-invasive ventilation, or MV.
Results: Of 2446 respiratory samples investigated during the study period, 514 from 430 patients were positive for P. jirovecii. Of these 430 patients, 107 met criteria for PJP and were included in the study, 53 (49.5%) patients had severe PJP, including 30 who required MV. All patients were immunocompromised with haematological malignancy ranking first (n = 37, 35%), followed by solid organ transplantation (n = 27, 25%), HIV-infection (n = 21, 20%), systemic diseases (n = 13, 12%), solid tumors (n = 12, 11%) and primary immunodeficiency (n = 6, 8%). By multivariate analysis, factors independently associated with severity were older age (OR, 3.36; 95% CI 1.4-8.5; p < 0.05), a P. jirovecii microscopy-positive result from bronchoalveolar lavage (BAL) (OR, 1.3; 95% CI 1.54-9.3; p < 0.05); and absence of a BAL fluid alveolitis profile (OR, 3.2; 95% CI 1.27-8.8; p < 0.04). The 90-day mortality rate was 27%, increasing to 50% in the severe PJP group. Factors independently associated with 90-day mortality were worse SOFA score on day 1 (OR, 1.05; 95% CI 1.02-1.09; p < 0.001) whereas alveolitis at BAL was protective (OR, 0.79; 95% CI 0.65-0.96; p < 0.05). In the subgroup of HIV-negative patients, similar findings were obtained, then viral co-infection were independently associated with higher 90-day mortality (OR, 1.25; 95% CI 1.02-1.55; p < 0.05).
Conclusions: Older age and P. jirovecii oocysts at microscopic examination of BAL were independently associated with severe PJP. Both initial PJP severity as evaluated by the SOFA score and viral co-infection predicted 90-day mortality. Alveolitis at BAL examination was associated with less severe PJP. The pathophysiological mechanism underlying this observation deserves further investigation.
Keywords: Alveolitis; Early prognostic score; Haematological malignancies; High flow oxygen; Pneumocystis jirovecii pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Winthrop KL, Novosad SA, Baddley JW, Calabrese L, Chiller T, Polgreen P, et al. Opportunistic infections and biologic therapies in immune-mediated inflammatory diseases: consensus recommendations for infection reporting during clinical trials and postmarketing surveillance. Ann Rheum Dis. 2015;74(12):2107–2116. doi: 10.1136/annrheumdis-2015-207841. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
