

Survey of non-resuscitation fluids administered during septic shock: a multicenter prospective observational study
- PMID: 31776712
- PMCID: PMC6881490
- DOI: 10.1186/s13613-019-0607-7
Survey of non-resuscitation fluids administered during septic shock: a multicenter prospective observational study
Abstract
Background: The indication, composition and timing of administration of non-resuscitation fluid in septic shock have so far received little attention and accordingly the potential to reduce this source of fluid is unknown. The objective of the study was to quantify and characterize non-resuscitation fluid administered to patients with septic shock.
Methods: This prospective observational study was performed in eight intensive care units in Sweden and Canada during 4 months in 2018. Adult patients with septic shock within 24 h of admission to the intensive care unit were eligible for inclusion. Non-resuscitation fluids were defined as fluids other than colloids, blood products and crystalloids at a rate ≥ 5 ml/kg/h. Indication, volume and type of fluid were recorded during the first 5 days after admission. A maximum of 30 patients could be included per centre. To estimate the potential to reduce administration of non-resuscitation fluid, a pragmatic "restrictive" protocol for administration of non-resuscitation fluids was devised based on the most restrictive practice already in place for non-resuscitation fluids at any of the participating centres. Data are presented as median (interquartile range [IQR]).
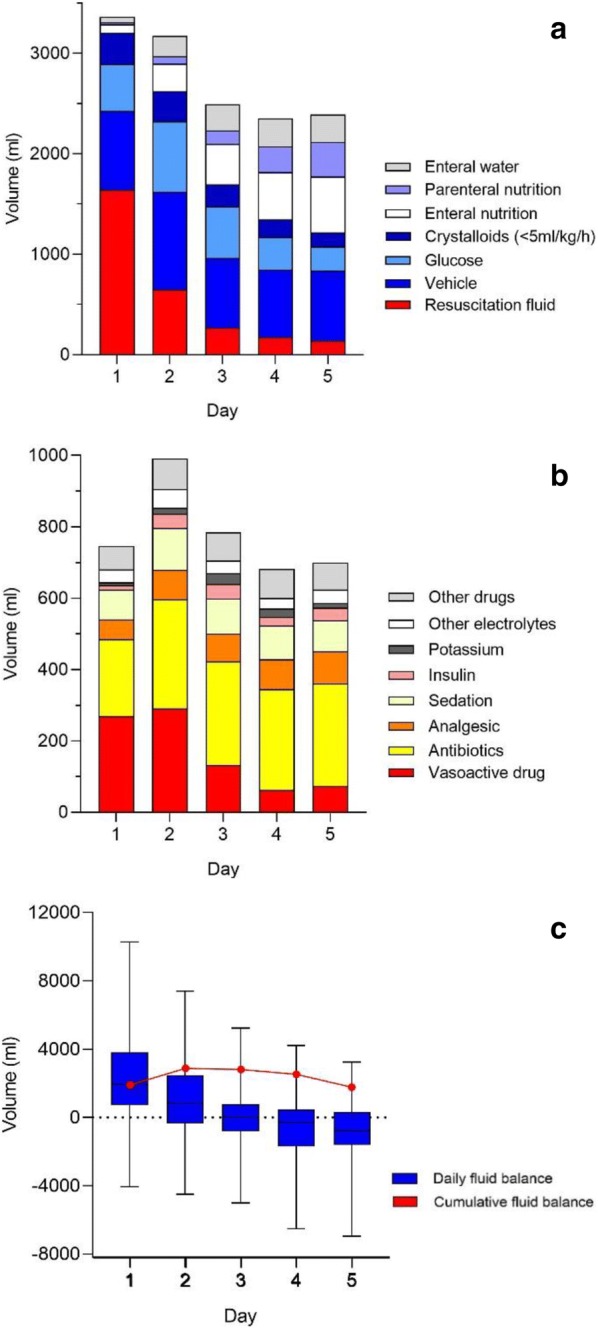
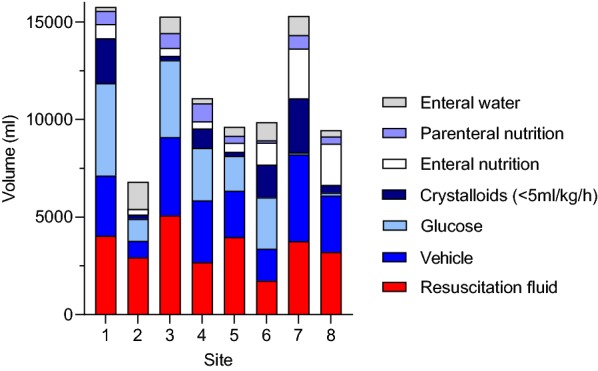
Results: A total of 200 patients were included in the study and the 30-day mortality was 35%. Patients received a total of 7870 (4060-12,340) ml of non-resuscitation fluids and 2820 (1430-4580) of resuscitation fluids during the observation period. Median volumes of non-resuscitation and resuscitation fluids were similar at day 1 (1620 [710-2320] and 1590 [520-3000]) ml, respectively) and non-resuscitation fluids represented the largest source of fluid from day 2 and onwards after admission to the ICU. Vehicles for drugs such as vasoactive drugs and antibiotics constituted the largest fraction of non-resuscitation fluids (2400 [1270-4030] ml) during the 5-day observation period. Modelling suggested that volume of non-resuscitation fluids could be reduced by 2840 (1270-4900) ml during the first 5 days of admission to the ICU, mainly through reducing maintenance fluids.
Conclusions: Non-resuscitation fluids constitute the major fraction of fluids administered in the ICU to patients suffering from septic shock and may represent the largest modifiable target to reduce fluid overload.
Keywords: Fluid balance; Non-resuscitation fluids; Septic shock; Vehicle.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
