

Epidemiology, clinical features, and management of severe hypercalcemia in critically ill patients
- PMID: 31776814
- PMCID: PMC6881488
- DOI: 10.1186/s13613-019-0606-8
Epidemiology, clinical features, and management of severe hypercalcemia in critically ill patients
Abstract
Background: Severe hypercalcemia (HCM) is a common reason for admission in intensive-care unit (ICU). This case series aims to describe the clinical and biological features, etiologies, treatments, and outcome associated with severe HCM. This study included all patients with a total calcemia above 12 mg/dL (3 mmol/L) admitted in two ICUs from January 2007 to February 2017.
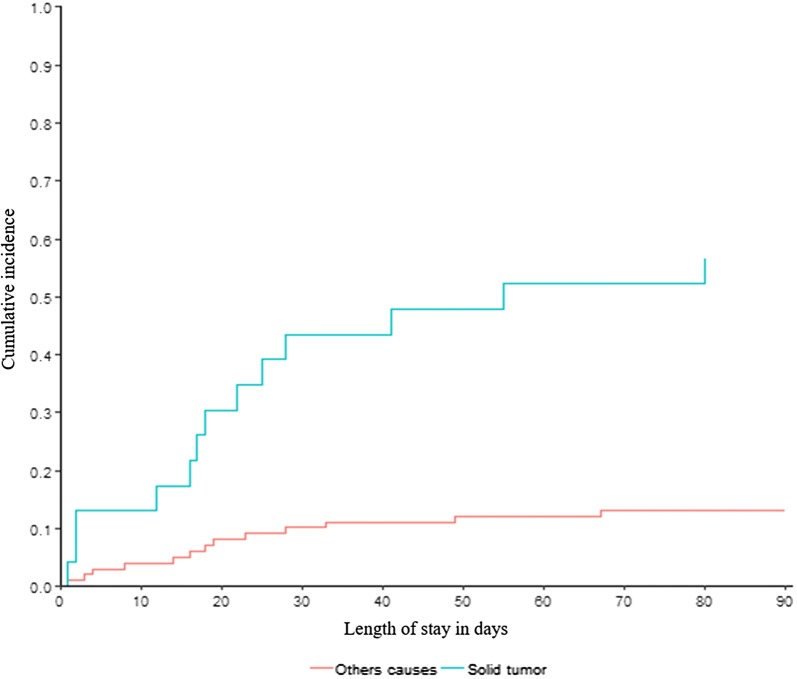
Results: 131 patients with HCM were included. HCM was related to hematologic malignancy in 58 (44.3%), solid tumors in 29 (22.1%), endocrinopathies in 16 (12.2%), and other causes in 28 (21.3%) patients. 108 (82.4%) patients fulfilled acute kidney injury (AKI) criteria. Among them, 25 (19%) patients required renal replacement therapy (RRT). 51 (38.9%) patients presented with neurological symptoms, 73 (55.7%) patients had cardiovascular manifestations, and 50 (38.1%) patients had digestive manifestations. The use of bisphosphonates (HR, 0.42; 95% CI, 0.27-0.67; P < 0.001) was the only treatment significantly associated with a decrease of total calcemia below 12 mg/dL (3 mmol/L) at day 5. ICU and Hospital mortality rates were, respectively, 9.9% and 21.3%. Simplified Acute Physiologic Score (SAPS II) (OR, 1.05; 95% CI 1.01-1.1; P = 0.03) and an underlying solid tumor (OR, 13.83; 95% CI 2.24-141.25; P = 0.01) were two independent factors associated with hospital mortality in multivariate analysis.
Conclusions: HCM is associated with high mortality rates, mainly due to underlying malignancies. The course of HCM may be complicated by organ failures which are most of the time reversible with early ICU management. Early ICU admission and prompt HCM management are crucial, especially in patients with an underlying solid tumor presenting with neurological symptoms.
Keywords: AKI etiology; Acute kidney injury (AKI); Hypercalcemia (HCM); Kidney disease outcome; Mortality; Onco-hematology; Prognosis; Renal replacement therapy (RRT).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ziegler R. Hypercalcemic Crisis. J Am Soc Nephrol. 2001;12(suppl 1):S3–S9. - PubMed
LinkOut - more resources
Full Text Sources
