

Patterns of Depressive Symptoms Before and After Surgery for Osteoarthritis: A Descriptive Study
- PMID: 31777796
- PMCID: PMC6857983
- DOI: 10.1002/acr2.1031
Patterns of Depressive Symptoms Before and After Surgery for Osteoarthritis: A Descriptive Study
Abstract
Objective: To examine patterns of depressive symptoms before and over the year following osteoarthritis (OA) surgery, stratified by joint and postsurgical outcome.
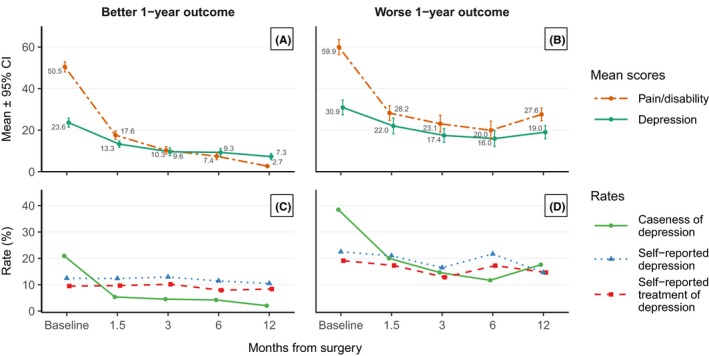
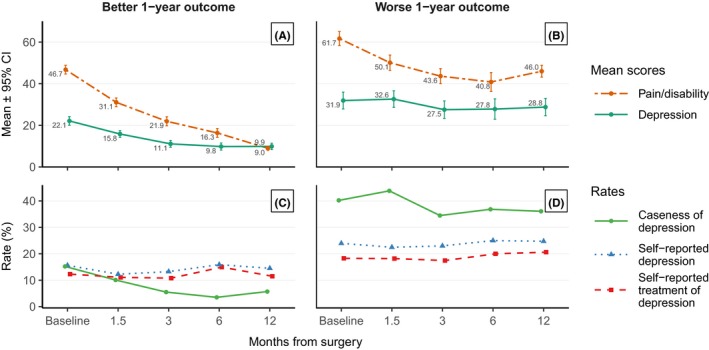
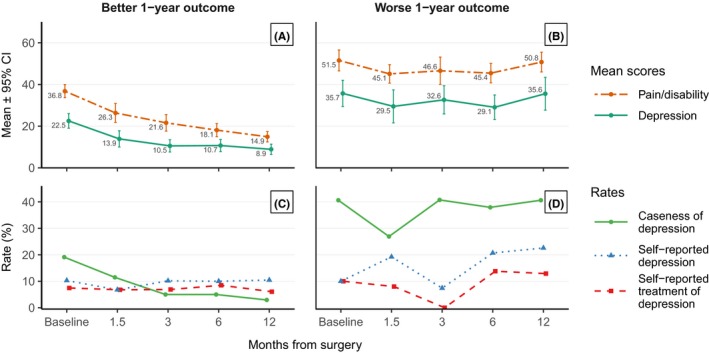
Methods: Participants were hip (n = 287), knee (n = 360), and lumbar spine (n = 100) OA patients scheduled for joint replacement or decompression surgery with or without fusion. One pre- and 4 postsurgery questionnaires were completed. Depressive symptoms were quantified using the Hospital Anxiety and Depression Scale (HADS). One-year outcomes were based on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scores for hip and knee patients and Oswestry Disability Index (ODI) scores for spine patients and were categorized as "worse" (top score tertile) vs. "better" outcomes (first, second tertiles). Plots over time were generated by joint and outcome: 1) mean pain/disability and depression scores and 2) percentage of patients meeting HADS cut-off for depression "caseness," reporting depression diagnosis and treatment.
Results: There were notable decreases in depression scores for patients with better outcomes. For those with worse outcomes, decreases were smaller for hip patients and were not significant for knee and spine patients. Among those with poorer outcomes, 25% of spine and knee patients were depression "cases" pre- and postsurgery; an additional 16% of spine and 10% of knee patients developed new "caseness" postsurgery. The proportion of these patients deemed depression cases by score was much higher than the proportion reporting diagnosis/treatment.
Conclusion: Although depressive symptoms decrease overall in OA patients postsurgery, degrees of change vary by joint and surgical outcome. Greater attention to mental health postsurgery is warranted and may lead to improved surgical outcomes, particularly among knee and spine patients.
© 2019 The Authors. ACR Open Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
Similar articles
-
The impact of multijoint symptoms on patient-reported disability following surgery for lumbar spine osteoarthritis.Spine J. 2021 Jan;21(1):80-89. doi: 10.1016/j.spinee.2020.08.005. Epub 2020 Aug 14. Spine J. 2021. PMID: 32805432
-
Sensitivity to Change of a Computer Adaptive Testing Instrument for Outcome Measurement After Hip and Knee Arthroplasty and Periacetabular Osteotomy.J Orthop Sports Phys Ther. 2016 Sep;46(9):756-67. doi: 10.2519/jospt.2016.6442. Epub 2016 Aug 5. J Orthop Sports Phys Ther. 2016. PMID: 27494055
-
Total joint replacement improves pain, functional quality of life, and health utilities in patients with late-stage knee and hip osteoarthritis for up to 5 years.Clin Rheumatol. 2020 Mar;39(3):861-871. doi: 10.1007/s10067-019-04811-y. Epub 2019 Nov 13. Clin Rheumatol. 2020. PMID: 31720892
-
Joint replacement surgery in elderly patients with severe osteoarthritis of the hip or knee: decision making, postoperative recovery, and clinical outcomes.Arch Intern Med. 2008 Jul 14;168(13):1430-40. doi: 10.1001/archinte.168.13.1430. Arch Intern Med. 2008. PMID: 18625924
-
Results of total joint arthroplasty and joint preserving surgery in younger patients evaluated by alternative outcome measures.Dan Med J. 2014 Apr;61(4):B4836. Dan Med J. 2014. PMID: 24814600 Review.
Cited by
-
Health, Psychological and Demographic Predictors of Depression in People with Fibromyalgia and Osteoarthritis.Int J Environ Res Public Health. 2022 Mar 14;19(6):3413. doi: 10.3390/ijerph19063413. Int J Environ Res Public Health. 2022. PMID: 35329109 Free PMC article.
-
Time course and correlates of psychological distress post spinal surgery: A longitudinal study.N Am Spine Soc J. 2023 Sep 14;16:100277. doi: 10.1016/j.xnsj.2023.100277. eCollection 2023 Dec. N Am Spine Soc J. 2023. PMID: 37869544 Free PMC article.
-
The Perioperative Symptom Severity of Higher Patient Health Questionnaire-9 Scores Between Genders in Single-Level Lumbar Fusion.Int J Spine Surg. 2021 Feb;15(1):62-73. doi: 10.14444/8007. Epub 2021 Feb 18. Int J Spine Surg. 2021. PMID: 33900958 Free PMC article.
-
The influence of peri-operative depressive symptoms on medium-term spine surgery outcome: a prospective study.Eur Spine J. 2023 Oct;32(10):3394-3402. doi: 10.1007/s00586-023-07875-2. Epub 2023 Aug 8. Eur Spine J. 2023. PMID: 37552328
-
Radiating pain during epidural needle insertion and catheter placement cannot be associated with postoperative persistent paresthesia: a retrospective review.JA Clin Rep. 2021 Aug 19;7(1):64. doi: 10.1186/s40981-021-00460-w. JA Clin Rep. 2021. PMID: 34410552 Free PMC article.
References
-
- Murray CJ, Lopez AD, World Health Organization , editors. The global burden of disease: a comprehensive assessment of the mortality and disability from diseases, injuries and frisk factors in 1990 and projected to 2020. Boston: Harvard School of Public Health on behalf of the World Health Organization and the the World Bank; 1996.
-
- Perruccio AV, Power JD, Badley EM. Revisiting arthritis prevalence projections–it's more than just the aging of the population. J Rheumatol 2006;33:1856–63. - PubMed
LinkOut - more resources
Full Text Sources
