

Review
doi: 10.1259/bjr.20190582.
Epub 2019 Dec 23.
Myths and realities of range uncertainty
Affiliations
- PMID: 31778317
- PMCID: PMC7066970
- DOI: 10.1259/bjr.20190582
Item in Clipboard
Review
Myths and realities of range uncertainty
Br J Radiol.
2020 Mar.
Abstract
Range uncertainty is a much discussed topic in proton therapy. Although a very real aspect of proton therapy, its magnitude and consequences are sometimes misunderstood or overestimated. In this article, the sources and consequences of range uncertainty are reviewed, a number of myths associated with the effect discussed with the aim of putting range uncertainty into clinical context and attempting to de-bunk some of the more exaggerated claims made as to its consequences.
Figures
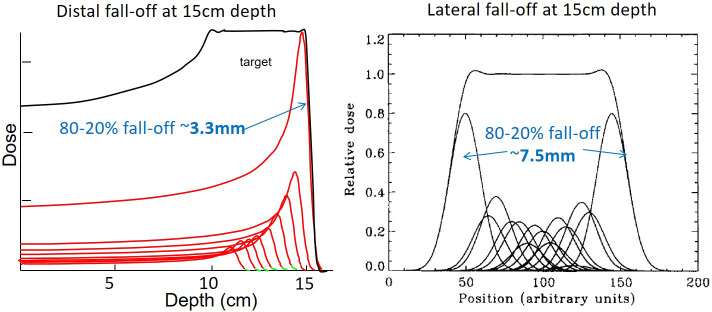
A comparison of distal and lateral fall-offs for PBS proton therapy in water. Both are for a Bragg peak depth of 15 cm in water. PBS,pencil beam scanning.
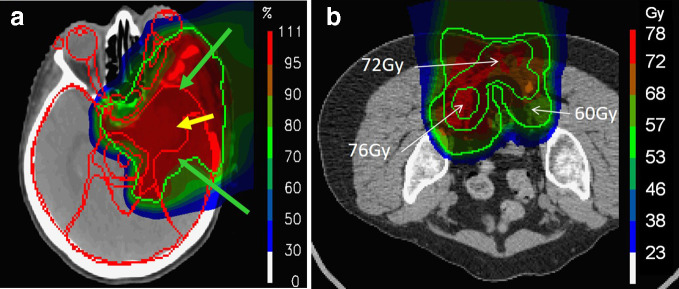
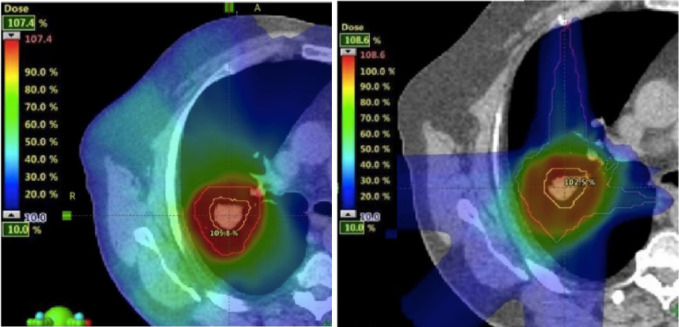
Example clinical dose distributions delivered at our institute using PBS proton therapy, showing the large volumes of normal tissue spared by the stopping characteristcis of protons. (a) A large meningioma treated using 3-fields. (b) A sacral chordoma treated with two posterior-oblique fields. PBS, pencil beam scanning.
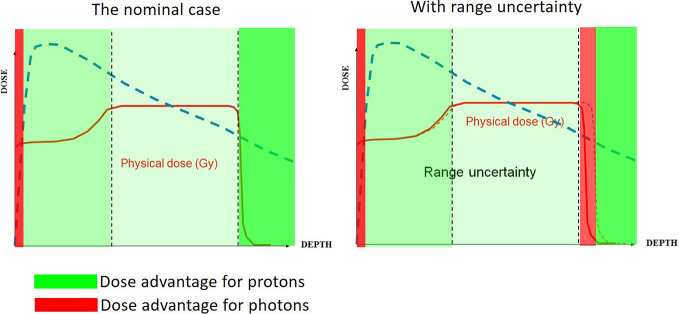
A schematic comparison of the dosimetric advantage of protons versus photons. (a) The nominal case (i.e. with perfectly accurate range), with the regions of dosimetric advantage of protons indicated in green. (b) The same comparison with an un-planned overshoot of the field.
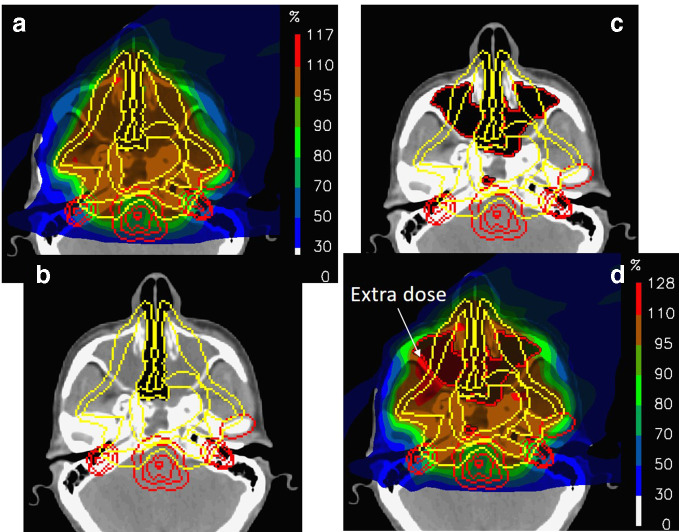
The dosimetric consequences of major changes in the filling of nasal cavities for a large chordoma in the paranasal region. (a) The nominal plan planned on the CT shown in (b). (c) New CT acquired on the first treatment day and the corresponding recalculated dose (d).
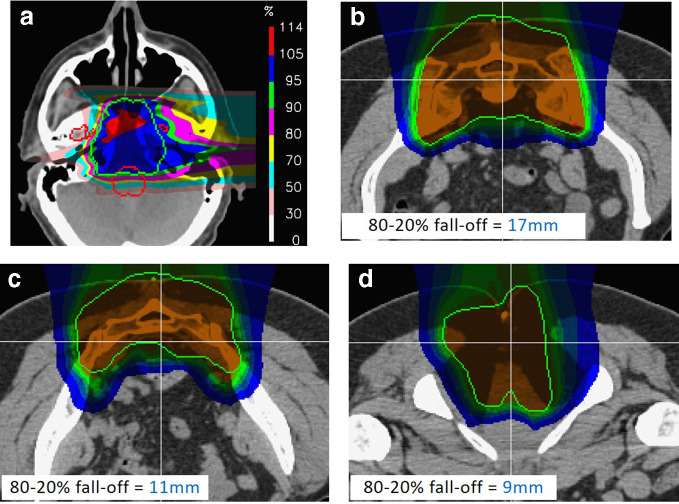
Realistic, in-vivo distal fall-offs for proton therapy. (a) For a single lateral field to a skull base chordoma. Note the extreme degradation of fall-off at the distal end due to density heterogeneities in the patient. (b–d). Example distal fall-offs to through different slices of the same sacral chordoma case. Note, all fall-offs are considerably larger than the distal fall-off shown in Figure 1.
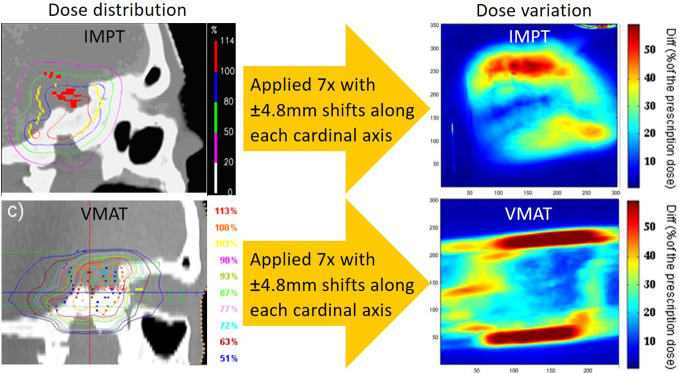
An experimental evaluation of plan robustness to set-up errors for VMAT and PBS proton therapy in an anthropomorphic phantom. Interestingly, the largest dose uncertainties are found at the lateral aspects of the VMAT plan even though this analysis inevitably includes the additional effects of set-up error induced range uncertainties for the proton plan. PBS,pencil beam scanning; VMAT, volumetric-modulated arc therapy.
A comparison between VMAT and PBS proton therapy to a Grade 1 NSCLC tumour. For the proton plan, field-specific range adapted PTV’s have been used in order to take into account range induced range changes. Even though such an approach somewhat mitigates the advantage of proton therapy, there is still a clear reduction of integral dose to the ipsi-lateral lung using protons. NSCLC,non-small-cell lung carcinoma; PBS, pencil beam scanning; PTV, planning targetvolume; VMAT, volumetric-modulated arc therapy.
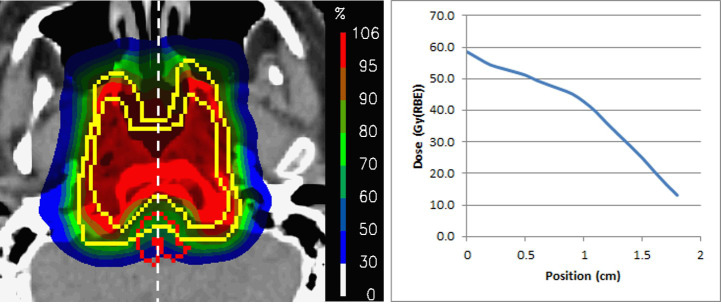
An example dose distribution to one of the 222 skull base chordomas reported by Weber et al. On the right is the dose profile along the white line from the anterior to posterior surface of the brainstem. Note the well-defined dose gradient across the organ, with the posterior surface receiving well under 20 Gy.
