

Automated measurement of liver attenuation to identify moderate-to-severe hepatic steatosis from chest CT scans
- PMID: 31778964
- PMCID: PMC7179816
- DOI: 10.1016/j.ejrad.2019.108723
Automated measurement of liver attenuation to identify moderate-to-severe hepatic steatosis from chest CT scans
Abstract
Purpose: Develop and validate an automated method for measuring liver attenuation in non-contrast low-dose chest CT (LDCT) scans and compare it to the standard manual method for identifying moderate-to-severe hepatic steatosis (HS).
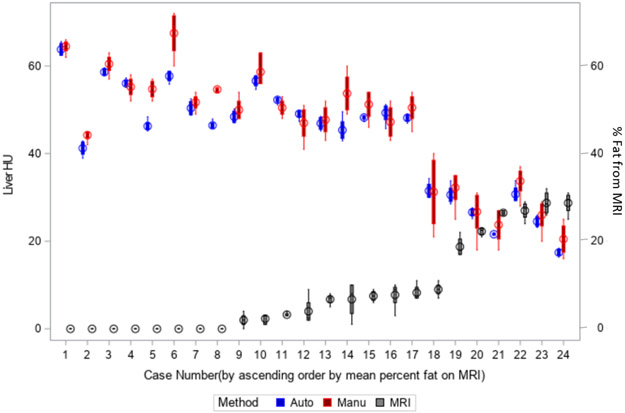
Method: The automated method identifies a region below the right lung within the liver and uses statistical sampling techniques to exclude non-liver parenchyma. The method was used to assess moderate-to-severe HS on two IRB-approved cohorts: 1) 24 patients with liver disease examined between 1/2013-1/2017 with non-contrast chest CT and abdominal MRI scans obtained within three months of liver biopsy, and 2) 319 lung screening participants with baseline LDCT performed between 8/2011-1/2017. Agreement between the manual and automated CT methods, the manual MRI method, and pathology for determining moderate-to-severe HS was assessed using Cohen's Kappa by applying a 40 HU threshold to the CT method and 17.4% fat fraction to MRI. Agreement between the manual and automated CT methods was assessed using the intraclass correlation coefficient (ICC). Variability was assessed using Bland-Altman limits of agreement (LoA).
Results: In the first cohort, the manual and automated CT methods had almost perfect agreement (ICC = 0.97, κ = 1.00) with LoA of -7.6 to 4.7 HU. Both manual and automated CT methods had almost perfect agreement with MRI (κ = 0.90) and substantial agreement with pathology (κ = 0.77). In the second cohort, the manual and automated CT methods had almost perfect agreement (ICC = 0.94, κ = 0.87). LoA were -10.6 to 5.2 HU.
Conclusion: Automated measurements of liver attenuation from LDCT scans can be used to identify moderate-to-severe HS on LDCT.
Keywords: Hepatic steatosis; Image analysis; Low-dose CT; Lung screening.
Copyright © 2019 Elsevier B.V. All rights reserved.
Figures















References
-
- Bedogni G, Miglioli L, Masutti F, Tiribelli C, Marchesini G, Bellentani S, Prevalence of and risk factors for nonalcoholic fatty liver disease: the Dionysos nutrition and liver study, Hepatology 42(1) (2005) 44–52. - PubMed
-
- Tang A, Desai A, Hamilton G, Wolfson T, Gamst A, Lam J, Clark L, Hooker J, Chavez T, Ang BD, Middleton MS, Peterson M, Loomba R, Sirlin CB, Accuracy of MR imaging-estimated proton density fat fraction for classification of dichotomized histologic steatosis grades in nonalcoholic fatty liver disease, Radiology 274(2) (2015) 416–25. - PMC - PubMed
-
- Noureddin M, Lam J, Peterson MR, Middleton M, Hamilton G, Le TA, Bettencourt R, Changchien C, Brenner DA, Sirlin C, Loomba R, Utility of magnetic resonance imaging versus histology for quantifying changes in liver fat in nonalcoholic fatty liver disease trials, Hepatology 58(6) (2013) 1930–40. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
