

A mixed methods process evaluation of a person-centred falls prevention program
- PMID: 31779624
- PMCID: PMC6883679
- DOI: 10.1186/s12913-019-4614-z
A mixed methods process evaluation of a person-centred falls prevention program
Erratum in
-
Correction: A mixed methods process evaluation of a person-centred falls prevention program.BMC Health Serv Res. 2023 Jun 27;23(1):695. doi: 10.1186/s12913-023-09743-7. BMC Health Serv Res. 2023. PMID: 37370149 Free PMC article. No abstract available.
Abstract
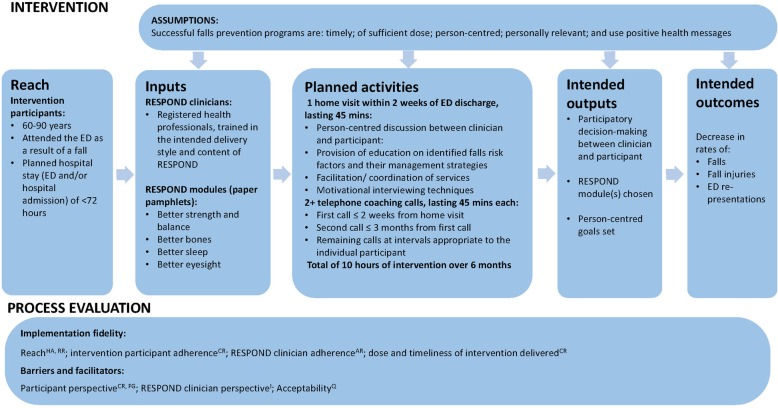
Background: RESPOND is a telephone-based falls prevention program for older people who present to a hospital emergency department (ED) with a fall. A randomised controlled trial (RCT) found RESPOND to be effective at reducing the rate of falls and fractures, compared with usual care, but not fall injuries or hospitalisations. This process evaluation aimed to determine whether RESPOND was implemented as planned, and identify implementation barriers and facilitators.
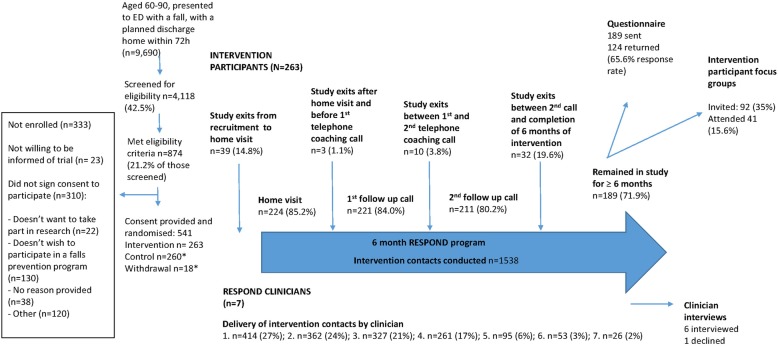
Methods: A mixed-methods evaluation was conducted alongside the RCT. Evaluation participants were the RESPOND intervention group (n = 263) and the clinicians delivering RESPOND (n = 7). Evaluation data were collected from participant recruitment and intervention records, hospital administrative records, audio-recordings of intervention sessions, and participant questionnaires. The Rochester Participatory Decision-Making Scale (RPAD) was used to evaluate person-centredness (score range 0 (worst) - 9 (best)). Process factors were compared with pre-specified criteria to determine implementation fidelity. Six focus groups were held with participants (n = 41), and interviews were conducted with RESPOND clinicians (n = 6). Quantitative data were analysed descriptively and qualitative data thematically. Barriers and facilitators to implementation were mapped to the 'Capability, Opportunity, Motivation - Behaviour' (COM-B) behaviour change framework.
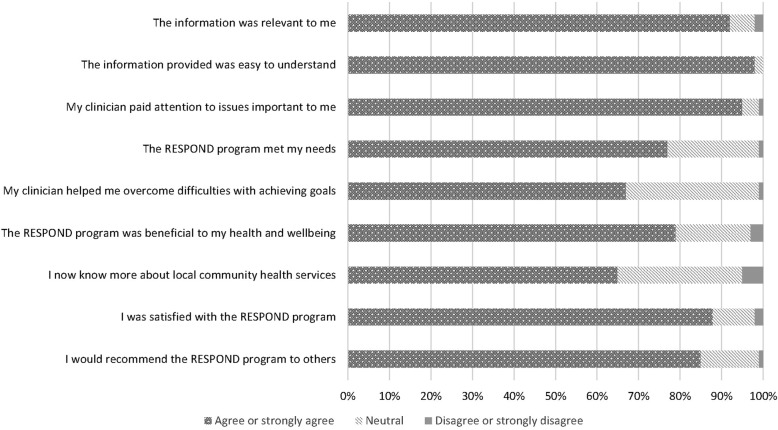
Results: RESPOND was implemented at a lower dose than the planned 10 h over 6 months, with a median (IQR) of 2.9 h (2.1, 4). The majority (76%) of participants received their first intervention session within 1 month of hospital discharge with a median (IQR) of 18 (12, 30) days. Clinicians delivered the program in a person-centred manner with a median (IQR) RPAD score of 7 (6.5, 7.5) and 87% of questionnaire respondents were satisfied with the program. The reports from participants and clinicians suggested that implementation was facilitated by the use of positive and personally relevant health messages. Complex health and social issues were the main barriers to implementation.
Conclusions: RESPOND was person-centred and reduced falls and fractures at a substantially lower dose, using fewer resources, than anticipated. However, the low dose delivered may account for the lack of effect on falls injuries and hospitalisations. The results from this evaluation provide detailed information to guide future implementation of RESPOND or similar programs.
Trial registration: This study was registered with the Australian New Zealand Clinical Trials Registry, number ACTRN12614000336684 (27 March 2014).
Keywords: Falls prevention; emergency department; fractures; older adults; process evaluation, complex intervention, mixed methods.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Salter A, Khan KM, Donaldson M, Davis J, Buchanan J, Abu-Laban RB, Cook WL, Lord SR, McKay HA. Community-dwelling seniors who present to the emergency department with a fall do not receive guideline care and their fall risk profile worsens significantly: a 6-month prospective study. Osteoporos Int. 2006;17(5):672–683. doi: 10.1007/s00198-005-0032-7. - DOI - PubMed
-
- Russell MA, Hill KD, Day LM, Blackberry I, Schwartz J, Giummarra MJ, Dorevitch M, Ibrahim JE, Dalton AC, Dharmage SC. A randomized controlled trial of a multifactorial falls prevention intervention for older fallers presenting to emergency departments. J Am Geriatr Soc. 2010;58(12):2265–2274. doi: 10.1111/j.1532-5415.2010.03191.x. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
