

Multiple Simultaneous Rare Distant Metastases as the Initial Presentation of Papillary Thyroid Carcinoma: A Case Report
- PMID: 31781034
- PMCID: PMC6856955
- DOI: 10.3389/fendo.2019.00759
Multiple Simultaneous Rare Distant Metastases as the Initial Presentation of Papillary Thyroid Carcinoma: A Case Report
Abstract
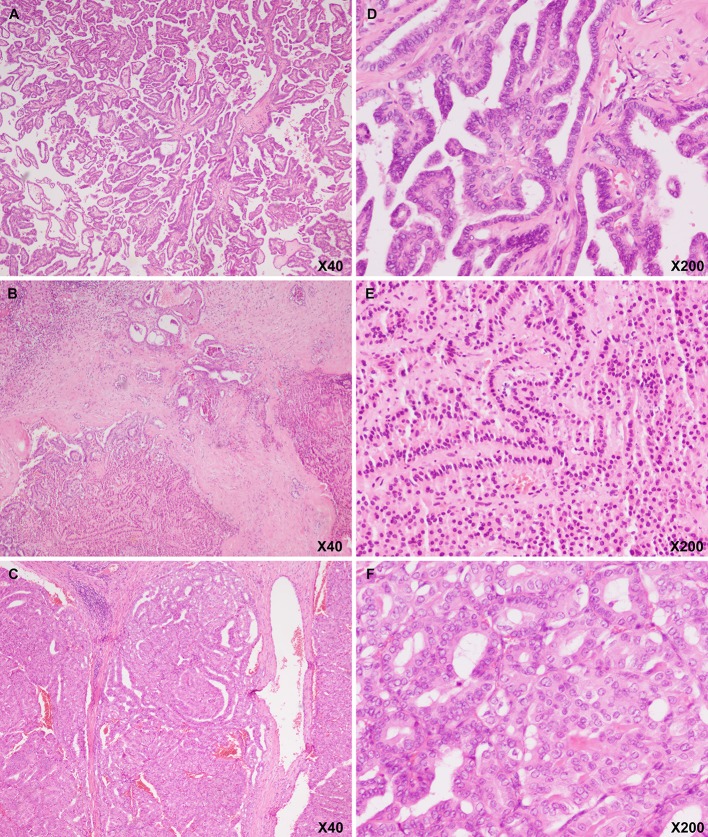
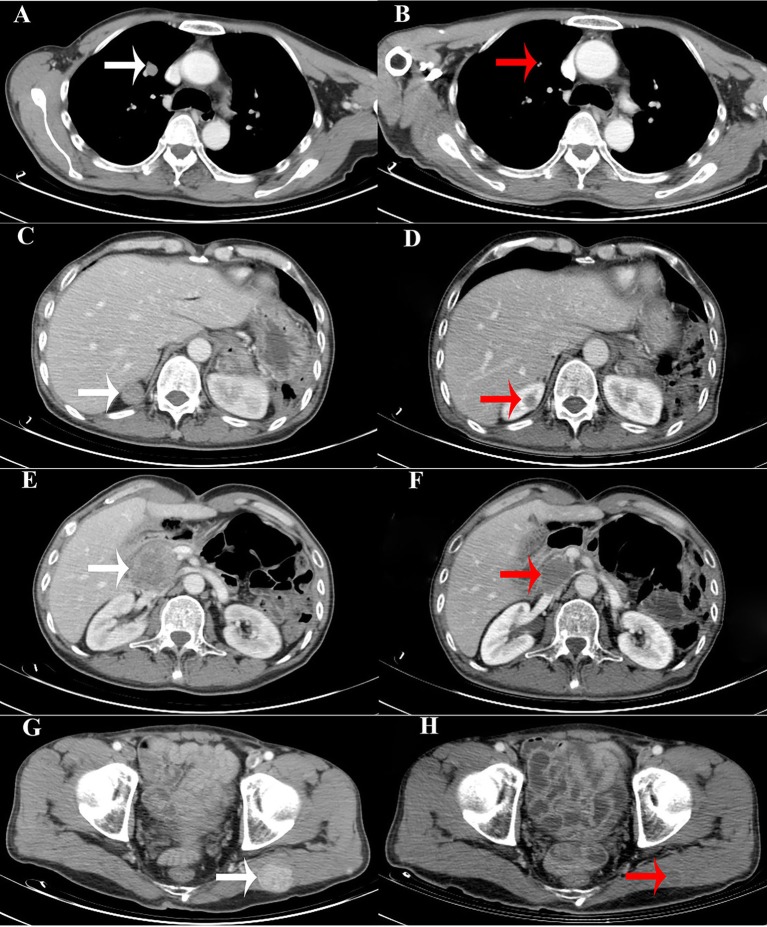
Papillary thyroid carcinoma (PTC) commonly metastasizes to regional lymph nodes. However, they infrequently cause rare distant metastases (RDMs), with the exclusion of lungs and bone metastases. RDMs are seldom identified prior to a primary thyroid cancer diagnosis. Therefore, cases initially presenting with synchronously multiple RDMs from PTC are extremely infrequent. This is a rare case of a 48-year-old man with initial diaphragm, pancreatic, and liver tumors from PTC. Following resection of the tumors, an ultrasound-guided fine-needle aspiration (US-FNA) cytology of a mass in the thyroid's left lobe revealed PTC. After postoperative recovery for more than 4 months, physical examination identified an irregular large nodule in the thyroid's isthmus and left lobe, a swollen lymph node in the left neck, and a mass in the right parotid gland. Ultrasound reexamination revealed numerous hypoechoic masses as follows: one in the thyroid's isthmus and entire left lobe (7.3 × 5.9 × 5.1 cm) and multiple in the thyroid's right lobe (0.2-0.3 cm). Ultrasound examination also showed several swollen lymph nodes in the left neck, a mass in the left gluteus maximus, and several masses in both the bilateral parotid and salivary region. The US-FNA's pathological examination confirmed metastatic PTCs in the left gluteus maximus and bilaterally located in the parotid and salivary gland. 18-fluorodeoxyglucose positron-emission tomography and computed tomography scan revealed abnormal uptakes in numerous locations (e.g., the thyroid's isthmus and left lobe, bilateral parotid gland, subcutaneous tissues, etc.). The patient underwent palliative therapy, including total thyroidectomy, bilateral central neck dissection, left lateral neck dissection, and excision of the bilateral parotid and salivary gland. A whole-body scan post-therapeutic radioactive iodine ablation showed exclusive thyroid bed uptake. Subsequently, the patient underwent continuous thyroid stimulating hormone repression therapy and was treated with lenvatinib chemotherapy for ~8 months. The primary thyroid tumor, pancreatic metastasis, and cervical lymph node metastasis were both positive for BRAF V600E and TERT promoter (C288T) mutations. After 13 months of follow-up, the patient is currently in stable clinical conditions. In conclusion, the present case is an extremely rare occurrence of simultaneous multiple RDMs from PTC as the initial presentation.
Keywords: 18F-FDG-PET/CT; PTC; chemotherapy; palliative therapy; rare distant metastases.
Copyright © 2019 Yang, Ma, Gong, Gong, Li and Zhu.
Figures

Similar articles
-
Case Report: A New Entity: Multiple Differentiated Variant of Papillary Thyroid Carcinoma With Advanced Clinical Behavior.Front Endocrinol (Lausanne). 2021 Apr 7;12:654638. doi: 10.3389/fendo.2021.654638. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33897621 Free PMC article.
-
Pancreatic metastasis arising from a BRAF(V600E)-positive papillary thyroid cancer: the role of endoscopic ultrasound-guided biopsy and response to sorafenib therapy.Thyroid. 2012 May;22(5):536-41. doi: 10.1089/thy.2011.0247. Epub 2012 Mar 21. Thyroid. 2012. PMID: 22435913
-
Distant, solitary skeletal muscle metastasis in recurrent papillary thyroid carcinoma.Thyroid. 2011 Sep;21(9):1027-31. doi: 10.1089/thy.2010.0249. Epub 2011 Aug 11. Thyroid. 2011. PMID: 21834676
-
Unusual metastasis of papillary thyroid cancer to the pancreas, liver, and diaphragm: a case report with review of literature.BMC Surg. 2020 Apr 22;20(1):82. doi: 10.1186/s12893-020-00748-1. BMC Surg. 2020. PMID: 32321510 Free PMC article. Review.
-
Pancreatic metastasis of papillary thyroid carcinoma preoperatively diagnosed by endoscopic ultrasound-guided fine-needle aspiration biopsy: a case report with review of literatures.Clin J Gastroenterol. 2018 Dec;11(6):521-529. doi: 10.1007/s12328-018-0875-z. Epub 2018 Jun 8. Clin J Gastroenterol. 2018. PMID: 29948817 Review.
Cited by
-
Dynamic Cancer Cell Heterogeneity: Diagnostic and Therapeutic Implications.Cancers (Basel). 2022 Jan 7;14(2):280. doi: 10.3390/cancers14020280. Cancers (Basel). 2022. PMID: 35053446 Free PMC article. Review.
-
Late Pancreatic Metastasis From Papillary Thyroid Carcinoma Diagnosed by Endoscopic Ultrasound-Guided Tissue Acquisition.Ochsner J. 2025 Summer;25(2):123-132. doi: 10.31486/toj.24.0115. Ochsner J. 2025. PMID: 40538612 Free PMC article.
-
Unusual metastases from differentiated thyroid cancers: A multicenter study in Korea.PLoS One. 2020 Aug 25;15(8):e0238207. doi: 10.1371/journal.pone.0238207. eCollection 2020. PLoS One. 2020. PMID: 32841270 Free PMC article.
-
Delving into the Role of lncRNAs in Papillary Thyroid Cancer: Upregulation of LINC00887 Promotes Cell Proliferation, Growth and Invasion.Int J Mol Sci. 2024 Jan 27;25(3):1587. doi: 10.3390/ijms25031587. Int J Mol Sci. 2024. PMID: 38338866 Free PMC article.
-
Papillary thyroid cancer with suspicious uterine cervix metastasis: a case report and literature review.Gland Surg. 2022 Jul;11(7):1270-1278. doi: 10.21037/gs-22-210. Gland Surg. 2022. PMID: 35935566 Free PMC article.
References
-
- SEER Preliminary Cancer Incidence Rate Estimates for 2017 and diagnosis years 2000 to 2017 SEER 18 Bethesda, MD: National Cancer Institute. https://seer.cancer.gov/statistics/preliminary-estimates/, based on the February 2019 SEER data submission and the November 2018 SEER data submission. Posted to the SEER web site, September 2019.
-
- Lloyd RV, Osamura RY, Klöppel G, Rosai J. editors. WHO Classification of Tumours of Endocrine Organs. 4th ed Lyon: IARC; (2017).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials