

Nomogram to Predict Internal Mammary Lymph Nodes Metastasis in Patients With Breast Cancer
- PMID: 31781496
- PMCID: PMC6857087
- DOI: 10.3389/fonc.2019.01193
Nomogram to Predict Internal Mammary Lymph Nodes Metastasis in Patients With Breast Cancer
Abstract
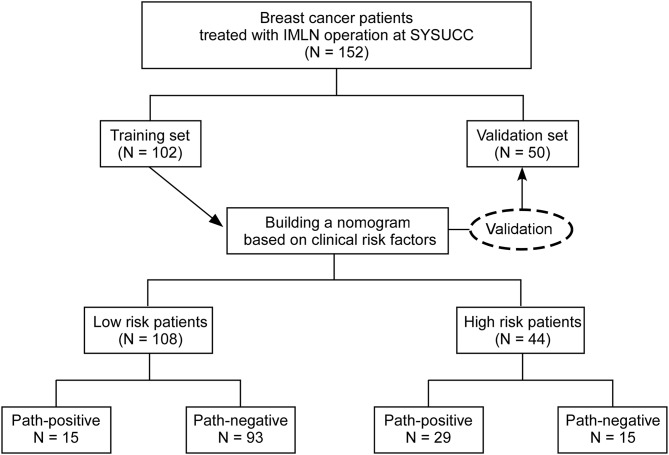
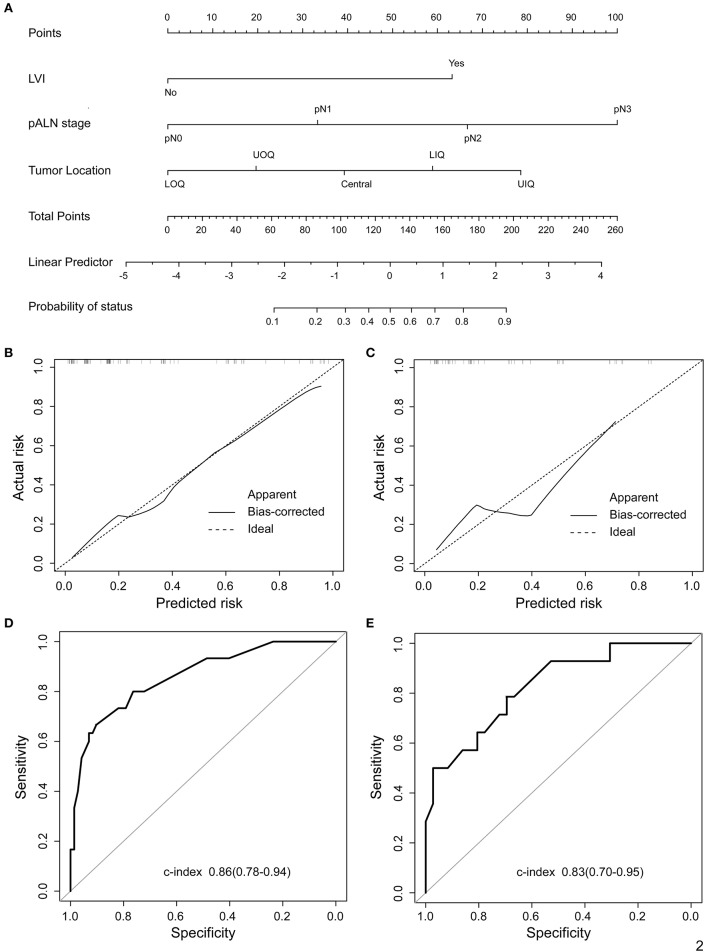
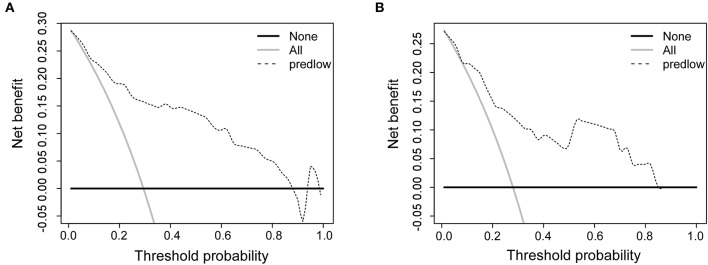
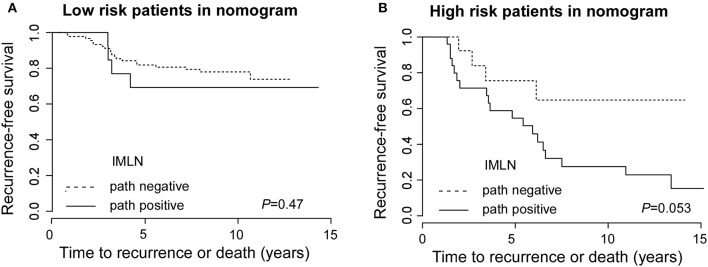
Background: Numerous studies have showed that internal mammary lymph node (IMLN) metastasis is an important adverse prognostic factor in patients with breast cancer (BC), however, there are no available prediction model for the preoperative diagnosis of IMLN metastasis. Methods: Data from 102 breast cancer patients treated with IMLN operation were used to establish and calibrate a nomogram for IMLN status based on multivariate logistic regression. Prediction performance of this model was further validated with a second set of 50 patients with BC. Discrimination of the predict model was assessed by the C-index, and calibration assessed by calibration plots. Moreover, we conducted the decision curve analysis (DCA) to evaluate the clinical value of the nomogram. Finally, the survival status of patients in different risk groups based on nomogram were also compared. Results: The final multivariate regression model included tumor location, lymph vascular invasion (LVI), and pathological axillary lymph node stage (pALN stage). A nomogram was developed as a graphical representation of the model and had good calibration and discrimination in both sets (with C-index of 0.86 and 0.83 for the training and validation set, respectively). Moreover, the DCA showed the clinical usefulness of our constructed nomogram. False negative (FN) in low risk group classified by nomogram (FN-LR-nomogram) did not significantly impact adjuvant treatment decision making, and more importantly, patients with FN-LR-nomogram had recurrence-free survival equivalent to patients with pathologically ture negative in low risk group classified by nomogram (TN-LR-nomogram). Conclusions: As a non-invasive prediction tool, our nomogram shows favorable predictive accuracy for IMLN metastasis in patients with BC and can serve as a basis to integrate future molecular markers for its clinical application.
Keywords: IMLN metastasis; breast cancer; nomogram; pALN stage; recurrence-free survival.
Copyright © 2019 Xie, Xiong, Li, Huang, Ye, Tang and Xie.
Figures
Similar articles
-
Predictors of internal mammary lymph nodes (IMLN) metastasis and disease-free survival comparison between IMLN-positive and IMLN-negative breast cancer patients: Results from Western China Clinical Cooperation Group (WCCCG) database (CONSORT).Medicine (Baltimore). 2018 Jul;97(28):e11296. doi: 10.1097/MD.0000000000011296. Medicine (Baltimore). 2018. PMID: 29995764 Free PMC article.
-
Preoperative Nomogram for Predicting Sentinel Lymph Node Metastasis Risk in Breast Cancer: A Potential Application on Omitting Sentinel Lymph Node Biopsy.Front Oncol. 2021 Apr 26;11:665240. doi: 10.3389/fonc.2021.665240. eCollection 2021. Front Oncol. 2021. PMID: 33981613 Free PMC article.
-
Elaboration and Validation of a Nomogram Based on Axillary Ultrasound and Tumor Clinicopathological Features to Predict Axillary Lymph Node Metastasis in Patients With Breast Cancer.Front Oncol. 2022 May 16;12:845334. doi: 10.3389/fonc.2022.845334. eCollection 2022. Front Oncol. 2022. PMID: 35651796 Free PMC article.
-
A validated web-based nomogram for predicting positive surgical margins following breast-conserving surgery as a preoperative tool for clinical decision-making.Breast. 2013 Oct;22(5):773-9. doi: 10.1016/j.breast.2013.01.010. Epub 2013 Feb 23. Breast. 2013. PMID: 23462681
-
Internal mammary lymph node metastases in breast cancer: what should radiologists know?Jpn J Radiol. 2018 Nov;36(11):629-640. doi: 10.1007/s11604-018-0773-9. Epub 2018 Sep 7. Jpn J Radiol. 2018. PMID: 30194586 Review.
Cited by
-
Comprehensive quantitative malignant risk prediction of pure grouped amorphous calcifications: clinico-mammographic nomogram.Quant Imaging Med Surg. 2022 May;12(5):2672-2683. doi: 10.21037/qims-21-797. Quant Imaging Med Surg. 2022. PMID: 35502394 Free PMC article.
-
Development and Validation of a Nomogram for Axillary Lymph Node Metastasis Risk in Breast Cancer.J Cancer. 2024 Oct 7;15(18):6122-6134. doi: 10.7150/jca.100651. eCollection 2024. J Cancer. 2024. PMID: 39440057 Free PMC article.
-
Clinical-radiomics model for predicting internal mammary lymph node metastasis in operable breast cancer patients.Front Oncol. 2025 Apr 3;15:1477866. doi: 10.3389/fonc.2025.1477866. eCollection 2025. Front Oncol. 2025. PMID: 40248206 Free PMC article.
-
Internal mammary lymph node metastasis in breast cancer patients based on anatomical imaging and functional imaging.Breast Cancer. 2022 Nov;29(6):933-944. doi: 10.1007/s12282-022-01377-7. Epub 2022 Jun 24. Breast Cancer. 2022. PMID: 35750935 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous