

Incidence and Mortality Trends and Risk Prediction Nomogram for Extranodal Diffuse Large B-Cell Lymphoma: An Analysis of the Surveillance, Epidemiology, and End Results Database
- PMID: 31781500
- PMCID: PMC6861389
- DOI: 10.3389/fonc.2019.01198
Incidence and Mortality Trends and Risk Prediction Nomogram for Extranodal Diffuse Large B-Cell Lymphoma: An Analysis of the Surveillance, Epidemiology, and End Results Database
Abstract
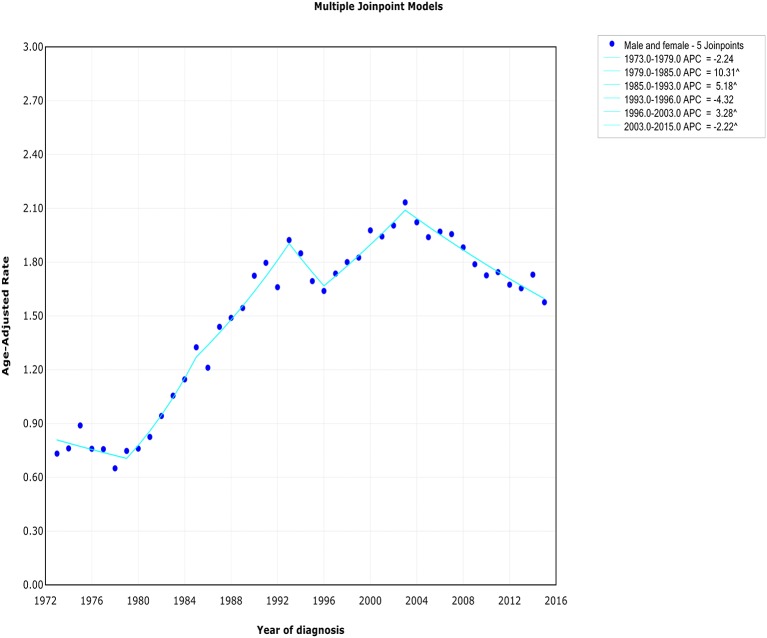
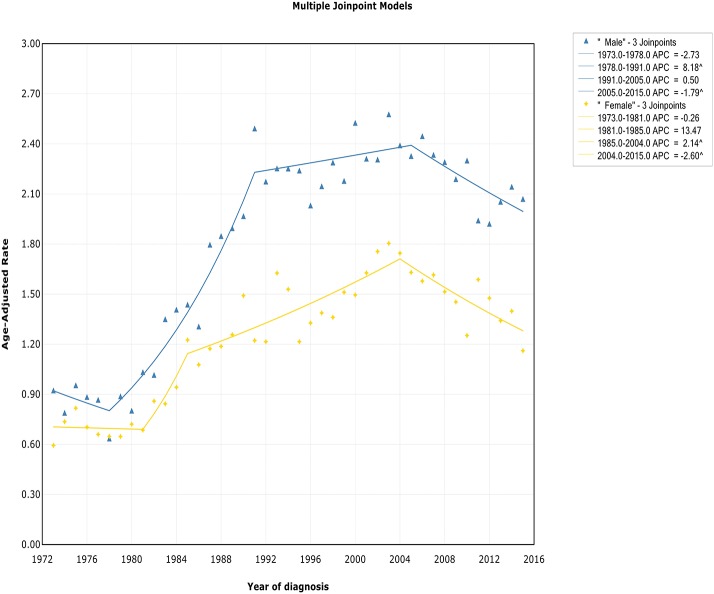
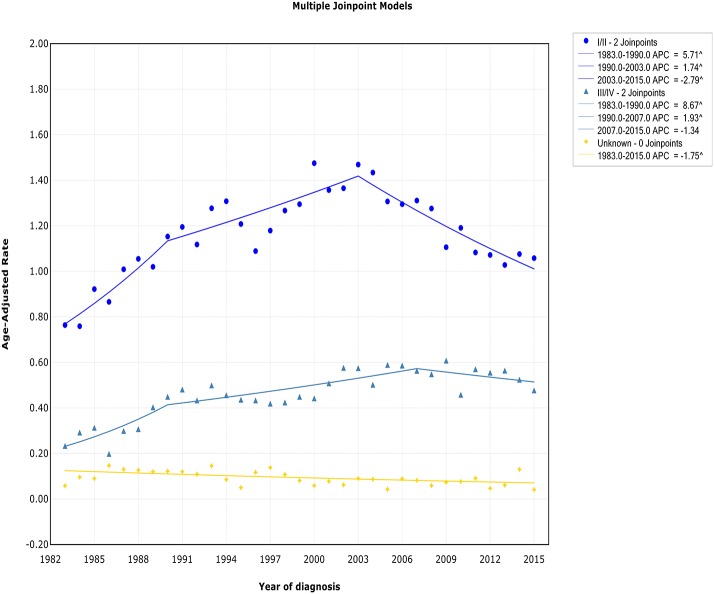
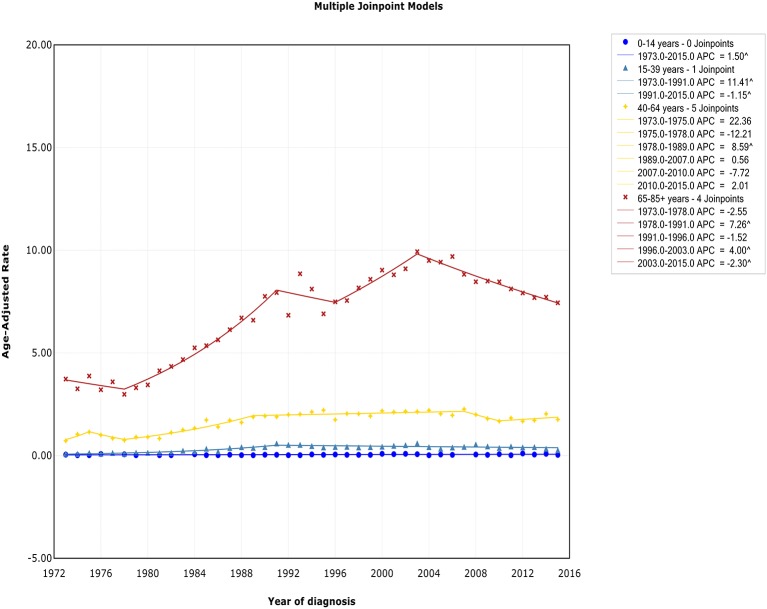
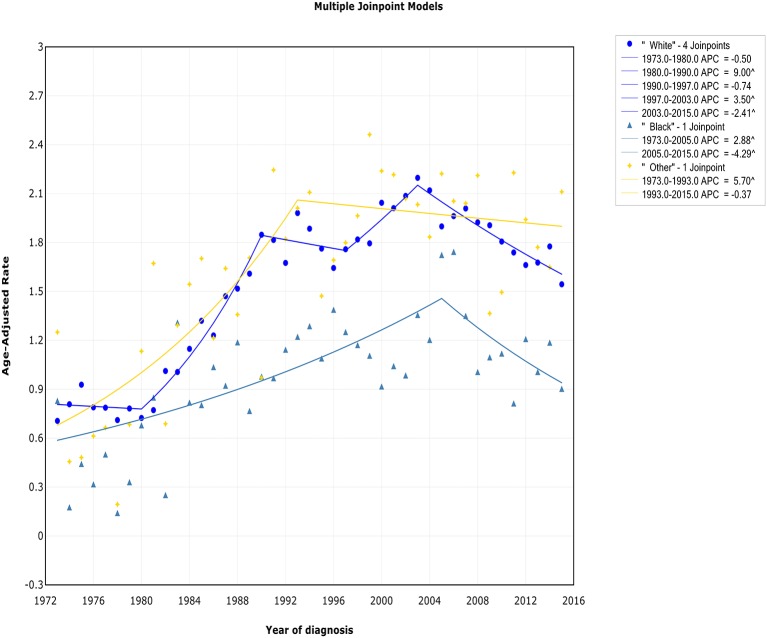
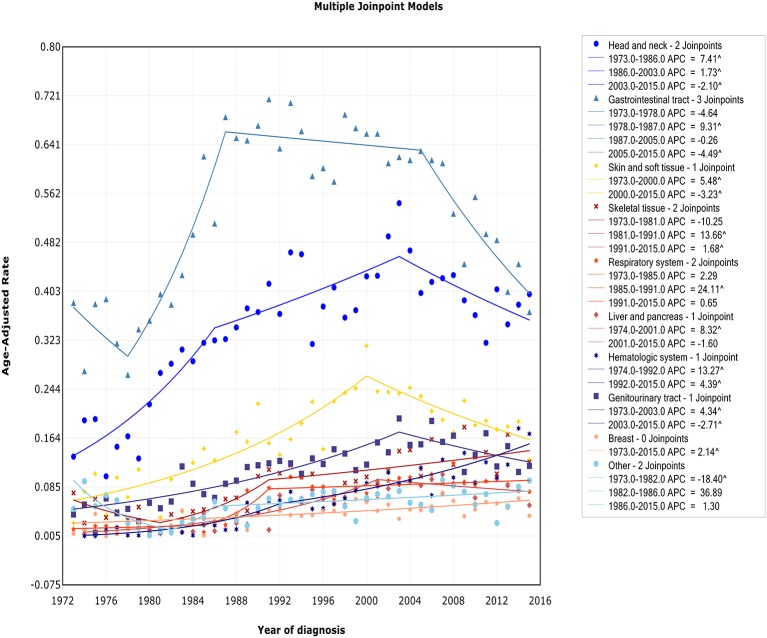
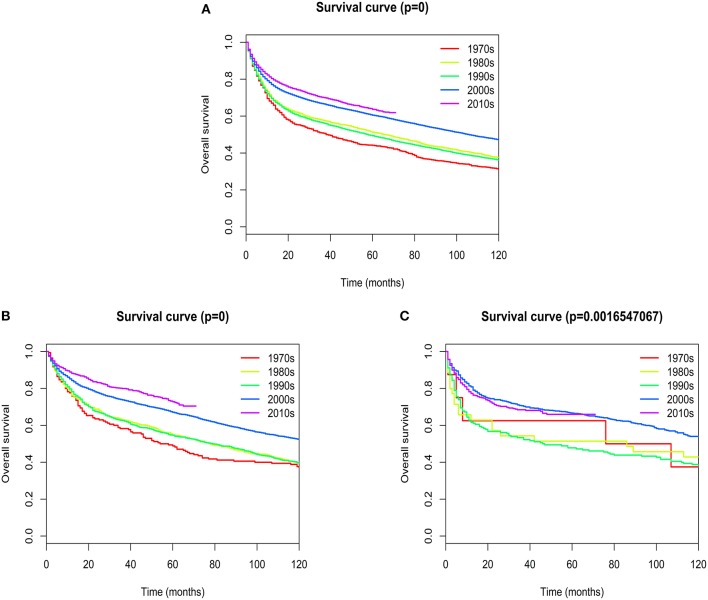
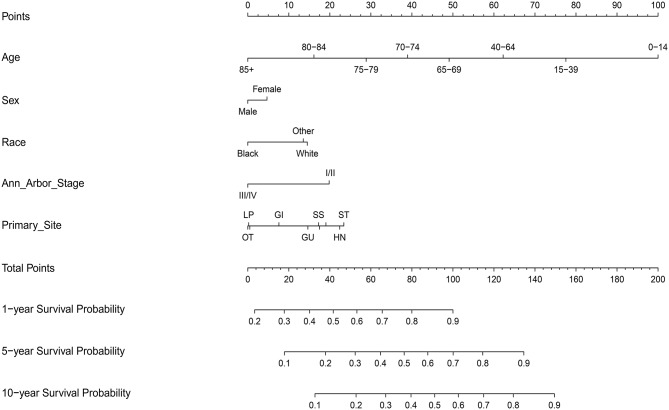
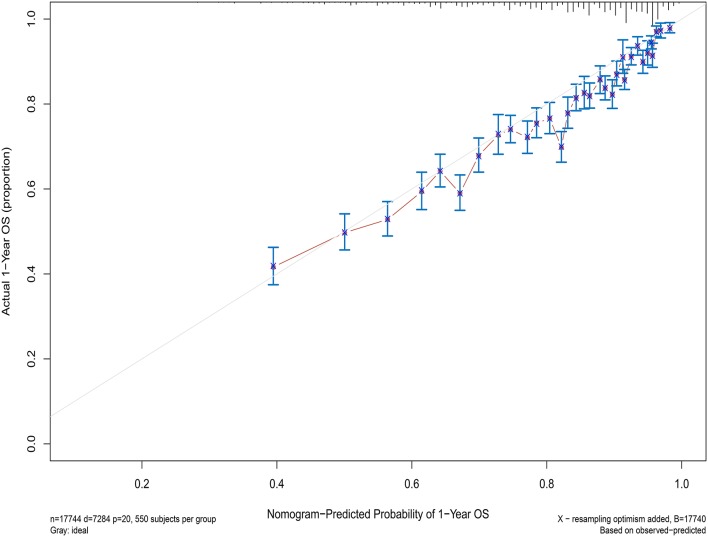
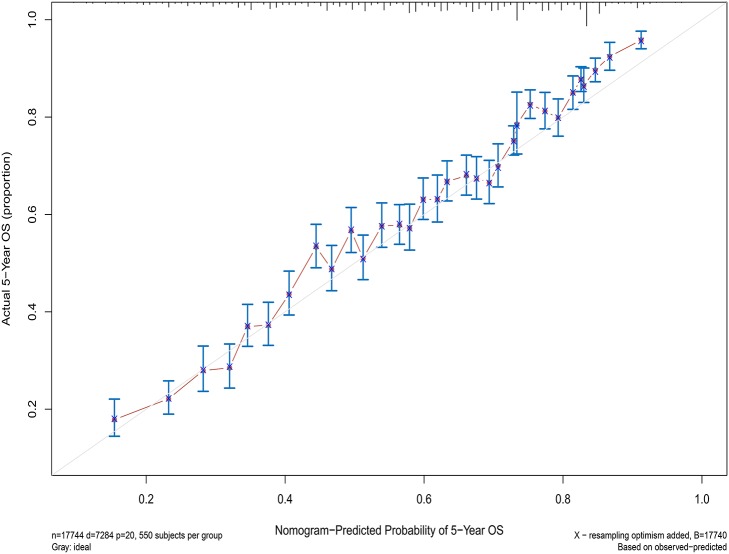
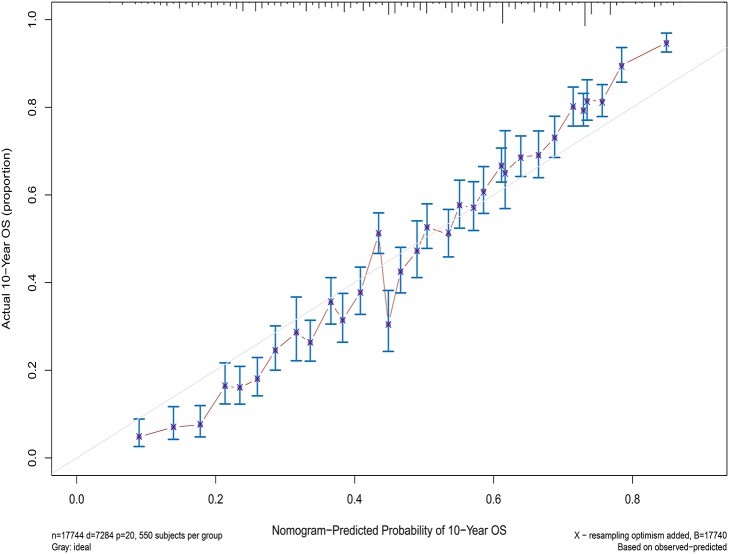
Background: DLBCL is the most commonly occurring type of non-Hodgkin's lymphoma, which may be found at various extranodal sites. But little is known about the particular trends of extranodal DLBCL. Methods: A total of 15,882 extranodal DLBCL patients were included in incidence analysis from the Surveillance, Epidemiology, and End Results (SEER) database (1973-2015). The joinpoint regression software was used to calculate the annual percent change (APC) in rates. Nomograms were established by R software to predict overall survival (OS). Results: The extranodal DLBCL incidence continued to rise at a rate of 1.6% (95% CI, 0.4-2.8, p < 0.001) per year over the study period, until it declined around 2003. The incidence-based mortality trend of extranodal DLBCL had a similar pattern, with a decrease happening around 1993. Five-year survival rates improved dramatically from the 1970s to 2010s (44.15 vs. 63.7%), and the most obvious increase occurred in DLBCL patients with primary site in the head/neck. The C-index showed a value for OS of 0.708, which validated the nomograms performed well and were able to forecast the prognosis of patients with extranodal DLBCL. The calibration curves showed satisfactory consistency between true values and predicted values for 1-, 5-, and 10-year overall survival, respectively. Conclusions: The incidence and incidence-based mortality of extranodal DLBCL had been increasing for decades, followed by a promising downward trend in recent years. These findings may help scientists identify disease-related risk factors and better manage the disease. The prediction signature cloud identifies high-risk patients who should receive effective therapies to prevent the fatal nature of this disease, and low-risk patients to reduce over-treatment.
Keywords: extranodal DLBCL; incidence; incidence-based mortality; nomograms; prognosis.
Copyright © 2019 Yin, Xu, Fan, Huang, Cheng, Zhang, Sun and Hu.
Figures
Similar articles
-
Prognostic factors and predictive models for primary pulmonary diffuse large B-cell lymphoma: a population-based analysis.Hematology. 2024 Dec;29(1):2420160. doi: 10.1080/16078454.2024.2420160. Epub 2024 Oct 28. Hematology. 2024. PMID: 39466076
-
Sites of extranodal involvement are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: an analysis of the Surveillance, Epidemiology and End Results database.Am J Hematol. 2014 Mar;89(3):310-4. doi: 10.1002/ajh.23638. Epub 2014 Feb 19. Am J Hematol. 2014. PMID: 24273125
-
The relationship among primary anatomic subsite and risk and distribution of second malignant neoplasms in patients with stage I/II diffuse large B-cell lymphoma: An analysis of the surveillance, epidemiology, and end results database.Transl Oncol. 2021 Jul;14(7):101106. doi: 10.1016/j.tranon.2021.101106. Epub 2021 Apr 28. Transl Oncol. 2021. PMID: 33932917 Free PMC article.
-
Extranodal Diffuse Large B Cell Lymphoma: Molecular Features, Prognosis, and Risk of Central Nervous System Recurrence.Curr Treat Options Oncol. 2018 Jun 21;19(8):38. doi: 10.1007/s11864-018-0555-8. Curr Treat Options Oncol. 2018. PMID: 29931605 Free PMC article. Review.
-
Diffuse large B-cell lymphoma.Crit Rev Oncol Hematol. 2013 Aug;87(2):146-71. doi: 10.1016/j.critrevonc.2012.12.009. Epub 2013 Jan 30. Crit Rev Oncol Hematol. 2013. PMID: 23375551 Review.
Cited by
-
Effect of surgical treatment for anorectal melanoma: a propensity score-matched analysis of the Surveillance, Epidemiology, and End Results programme data.BMJ Open. 2022 Apr 21;12(4):e053339. doi: 10.1136/bmjopen-2021-053339. BMJ Open. 2022. PMID: 35450893 Free PMC article.
-
A dynamic predictive nomogram of long-term survival in primary gastric lymphoma: a retrospective study.BMC Gastroenterol. 2022 Jul 16;22(1):347. doi: 10.1186/s12876-022-02419-2. BMC Gastroenterol. 2022. PMID: 35842604 Free PMC article.
-
Ferroptosis-Related Gene Signature: A New Method for Personalized Risk Assessment in Patients with Diffuse Large B-Cell Lymphoma.Pharmgenomics Pers Med. 2021 May 26;14:609-619. doi: 10.2147/PGPM.S309846. eCollection 2021. Pharmgenomics Pers Med. 2021. PMID: 34079336 Free PMC article.
-
CircPCBP2 promotes the stemness and chemoresistance of DLBCL via targeting miR-33a/b to disinhibit PD-L1.Cancer Sci. 2022 Aug;113(8):2888-2903. doi: 10.1111/cas.15402. Epub 2022 Jun 14. Cancer Sci. 2022. PMID: 35579082 Free PMC article.
-
A Novel Defined Super-Enhancer Associated Gene Signature to Predict Prognosis in Patients With Diffuse Large B-Cell Lymphoma.Front Genet. 2022 Jun 14;13:827840. doi: 10.3389/fgene.2022.827840. eCollection 2022. Front Genet. 2022. PMID: 35774514 Free PMC article.
References
-
- Fitzmaurice C, Akinyemiju TF, Al Lami FH, Alam T, Alizadeh-Navaei R, et al. . Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: a systematic analysis for the global burden of disease study. JAMA Oncol. (2018) 4:1553–68. 10.1200/JCO.2018.36.15_suppl.1568 - DOI - PMC - PubMed
-
- Morton LM, Turner JJ, Cerhan JR, Linet MS, Treseler PA, Clarke CA, et al. . Proposed classification of lymphoid neoplasms for epidemiologic research from the Pathology Working Group of the International Lymphoma Epidemiology Consortium (InterLymph). Blood. (2007) 110:695–708. 10.1182/blood-2006-11-051672 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources