

Clinics in diagnostic imaging (201). Small bowel intramural haematoma induced by anticoagulation therapy with associated reactive ileus
- PMID: 31781781
- PMCID: PMC6875801
- DOI: 10.11622/smedj.2019147
Clinics in diagnostic imaging (201). Small bowel intramural haematoma induced by anticoagulation therapy with associated reactive ileus
Abstract
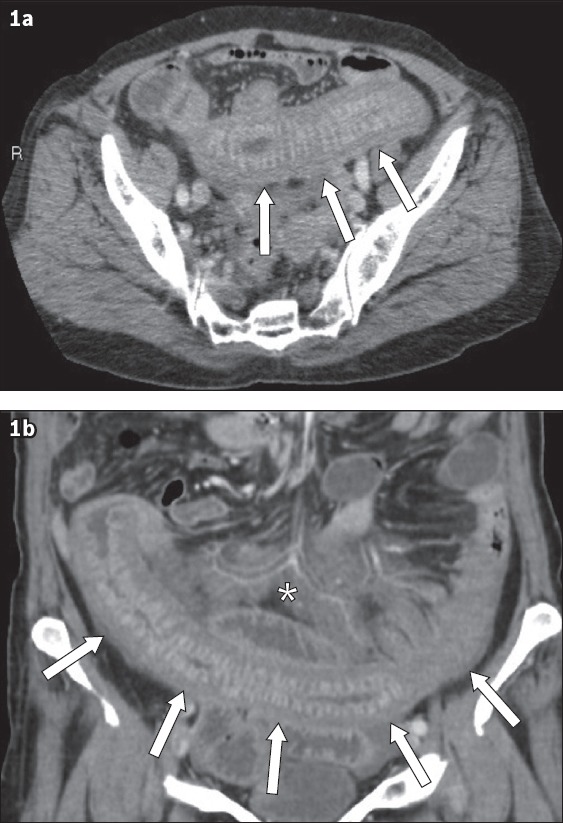
A 74-year-old woman receiving long-term anticoagulation with warfarin for chronic atrial fibrillation presented with severe acute abdominal pain, diarrhoea and vomiting. Initial laboratory workup revealed a deranged coagulation profile. Computed tomography of the abdomen and pelvis demonstrated spontaneous distal jejunal intramural haematoma with associated reactive ileus. No overt pneumatosis intestinalis, intraperitoneal free gas or haemoperitoneum was seen. Based on clinical and imaging findings, a diagnosis of over-anticoagulation complicated by small bowel intramural haematoma was made. The patient was managed non-operatively with analgesia, cessation of warfarin and reversal therapy with vitamin K. Warfarin therapy was recommenced upon resolution of symptoms and optimisation of coagulation status. The clinical presentation, radiological features and overall management of anticoagulation-induced bleeding are further discussed in this article.
Keywords: anticoagulants; atrial fibrillation; haematoma; haemorrhage; warfarin.
Copyright: © Singapore Medical Association.
Figures
Similar articles
-
Warfarin-induced spontaneous intramural small bowel hematoma presenting as an acute abdomen: A case report.Medicine (Baltimore). 2022 Sep 2;101(35):e30335. doi: 10.1097/MD.0000000000030319. Medicine (Baltimore). 2022. PMID: 36107558 Free PMC article.
-
Small bowel obstruction caused by intramural hemorrhage secondary to anticoagulant therapy.Acta Gastroenterol Belg. 2008 Jul-Sep;71(3):342-4. Acta Gastroenterol Belg. 2008. PMID: 19198584
-
[Spontaneous intramural hematoma of the small bowel due to use of oral anticoagulants: case report and review of the literature].Rev Gastroenterol Peru. 2010 Apr-Jun;30(2):158-62. Rev Gastroenterol Peru. 2010. PMID: 20644609 Review. Spanish.
-
Small bowel obstruction caused by intramural hematoma secondary to warfarin therapy: a report of two cases.Turk J Gastroenterol. 2011;22(2):199-202. doi: 10.4318/tjg.2011.0192. Turk J Gastroenterol. 2011. PMID: 21796559
-
Anticoagulant-induced intramural intestinal hematoma: report of three cases and literature review.J Med Assoc Thai. 2008 Aug;91(8):1285-90. J Med Assoc Thai. 2008. PMID: 18788704 Review.
Cited by
-
Warfarin-induced spontaneous intramural small bowel hematoma presenting as an acute abdomen: A case report.Medicine (Baltimore). 2022 Sep 2;101(35):e30335. doi: 10.1097/MD.0000000000030319. Medicine (Baltimore). 2022. PMID: 36107558 Free PMC article.
References
-
- Sorbello MP, Utiyama EM, Parreira JG, Birolini D, Rasslan S. Spontaneous intramural small bowel haematoma induced by anticoagulant therapy:review and case report. Clinics (Sao Paulo) 2007;62:785–90. - PubMed
-
- Shaw PH, Ranganathan S, Gaines B. A spontaneous intramural hematoma of the bowel presenting as obstruction in a child receiving low-molecular-weight heparin. J Pediatr Hematol Oncol. 2005;27:558–60. - PubMed
-
- Abbas MA, Collins JM, Olden KW. Spontaneous intramural small-bowel hematoma:imaging findings and outcome. AJR Am J Roentgenol. 2002;179:1389–94. - PubMed
-
- Abdel Samie A, Theilmann L. Detection and management of spontaneous intramural small bowel hematoma secondary to anticoagulant therapy. Expert Rev Gastroenterol Hepatol. 2012;6:553–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
