

Long-term remission of disseminated parathyroid cancer following immunotherapy
- PMID: 31782130
- PMCID: PMC9361402
- DOI: 10.1007/s12020-019-02136-z
Long-term remission of disseminated parathyroid cancer following immunotherapy
Abstract
Purpose: Parathyroid cancer is a rare tumor associated with poor prognosis particularly when disseminated. While chemotherapy and/or radiotherapy are of no clinical value in disseminated disease, immunotherapy should be considered.
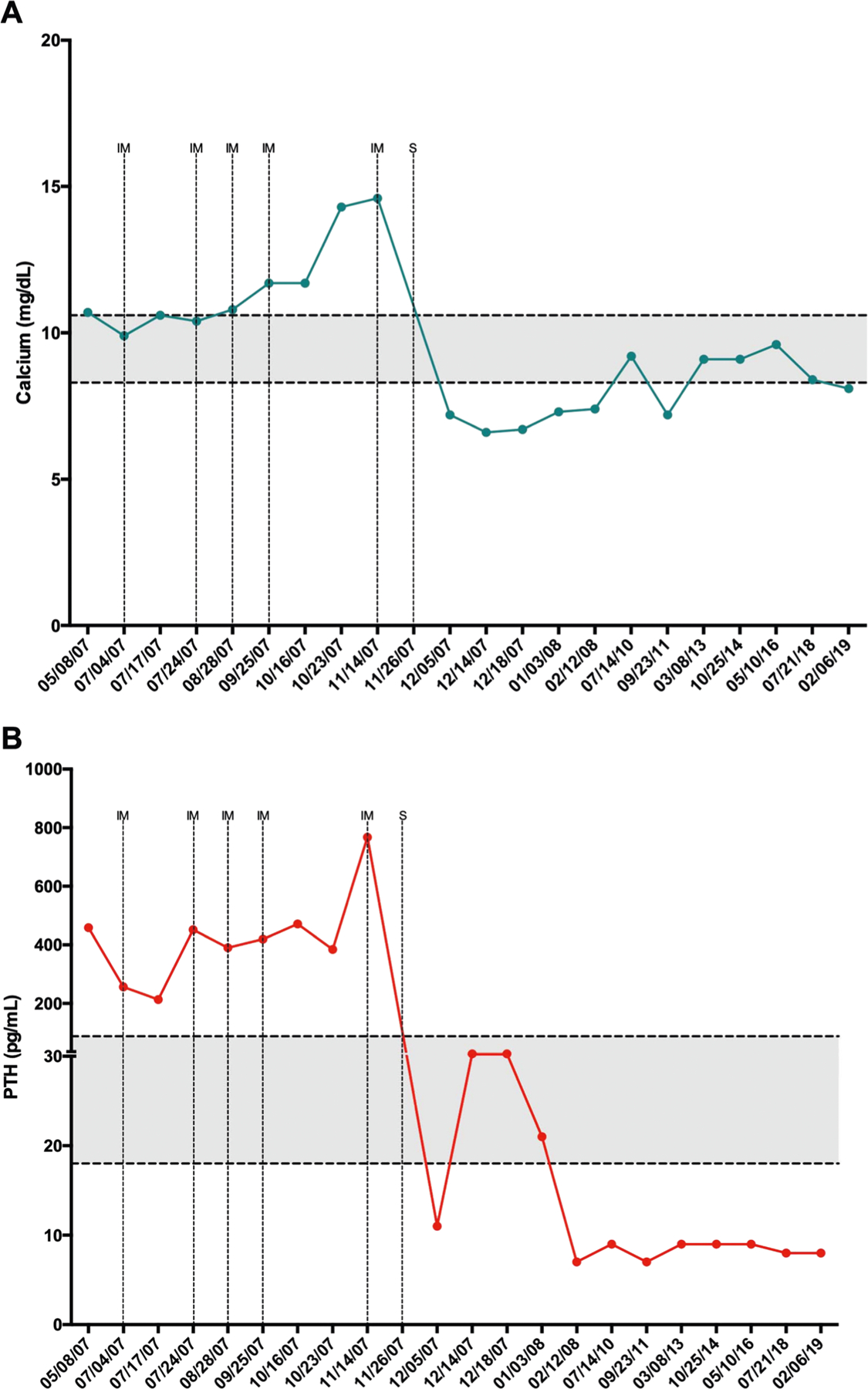
Subject and results: A patient with CDC73-associated metastatic parathyroid carcinoma was treated with combined anti-hPTH immunotherapy and surgery.
Conclusions: Following five courses of anti-hPTH immunotherapy and subsequent surgery, a 12-year long remission of disseminated parathyroid cancer is reported. This case further supports the ever-expanding spectrum of cancers that may benefit from immunotherapy.
Keywords: Cancer; Immunotherapy; Parathyroid.
Conflict of interest statement
Figures


References
-
- Sadler C, Sadler C, Gow KW, Beierle EA, Doski JJ, Langer M, Nuchtern JG, Vasudevan SA, Goldfarb M, Parathyroid carcinoma in more than 1,000 patients: a population-level analysis. Surgery 156, 1622–1629 (2014) - PubMed
-
- Betea D, Potorac I, Beckers A, Parathyroid carcinoma: challenges in diagnosis and treatment. Ann. Endocrinol 76, 169–177 (2015) - PubMed
-
- Salcuni AS, Cetani F, Guarnieri V, Nicastro V, Romagnoli E, de Martino D, Scillitani A, Cole DEC, Parathyroid carcinoma. Best Pract. Res. Clin. Endocrinol. Metab 32, 877–889 (2018) - PubMed
-
- Brewer K., J. Costa-Guda, A. Arnold, Molecular genetic insights into sporadic primary hyperparathyroidism. Endocr. Relat. Cancer 26, R53–R72 (2019) - PubMed
-
- Cavalier E, Daly AF, Betea D, Pruteanu-Apetrii PN, Delanaye P, Stubbs P, Bradwell AR, Chapelle JP, Beckers A, The ratio of parathyroid hormone as measured by third- and second-generation assays as a marker of parathyroid carcinoma. J. Clin. Endocrinol. Metab 95, 3745–3749 (2010) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
