

Phase I study of vorinostat with gefitinib in BIM deletion polymorphism/epidermal growth factor receptor mutation double-positive lung cancer
- PMID: 31782583
- PMCID: PMC7004511
- DOI: 10.1111/cas.14260
Phase I study of vorinostat with gefitinib in BIM deletion polymorphism/epidermal growth factor receptor mutation double-positive lung cancer
Abstract
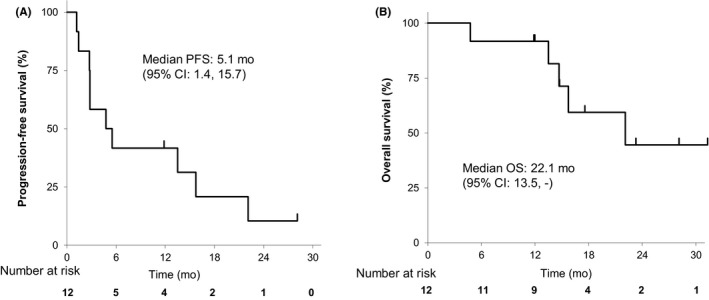
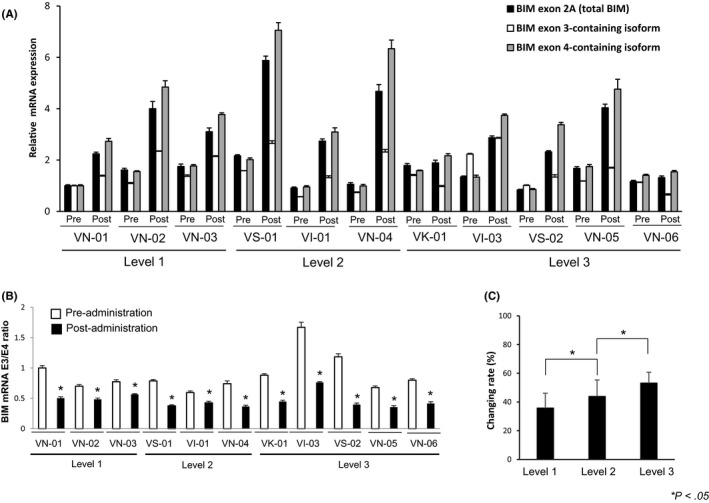
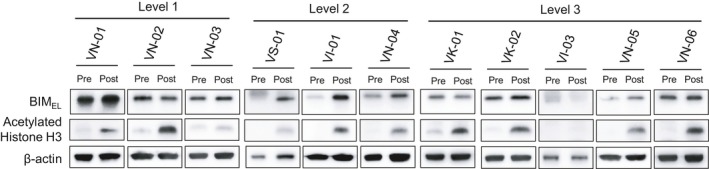
Patients with epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (NSCLC) harboring BIM deletion polymorphism (BIM deletion) have poor responses to EGFR TKI. Mechanistically, the BIM deletion induces preferential splicing of the non-functional exon 3-containing isoform over the functional exon 4-containing isoform, impairing TKI-induced, BIM-dependent apoptosis. Histone deacetylase inhibitor, vorinostat, resensitizes BIM deletion-containing NSCLC cells to EGFR-TKI. In the present study, we determined the safety of vorinostat-gefitinib combination and evaluated pharmacodynamic biomarkers of vorinostat activity. Patients with EGFR-mutated NSCLC with the BIM deletion, pretreated with EGFR-TKI and chemotherapy, were recruited. Vorinostat (200, 300, 400 mg) was given daily on days 1-7, and gefitinib 250 mg was given daily on days 1-14. Vorinostat doses were escalated based on a conventional 3 + 3 design. Pharmacodynamic markers were measured using PBMC collected at baseline and 4 hours after vorinostat dose on day 2 in cycle 1. No dose-limiting toxicities (DLT) were observed in 12 patients. We determined 400 mg vorinostat as the recommended phase II dose (RP2D). Median progression-free survival was 5.2 months (95% CI: 1.4-15.7). Disease control rate at 6 weeks was 83.3% (10/12). Vorinostat preferentially induced BIM mRNA-containing exon 4 over mRNA-containing exon 3, acetylated histone H3 protein, and proapoptotic BIMEL protein in 11/11, 10/11, and 5/11 patients, respectively. These data indicate that RP2D was 400 mg vorinostat combined with gefitinib in BIM deletion/EGFR mutation double-positive NSCLC. BIM mRNA exon 3/exon 4 ratio in PBMC may be a useful pharmacodynamic marker for treatment.
Keywords: BIM deletion polymorphism; EGFR-TKI; NSCLC; resistance; vorinostat.
© 2019 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Conflict of interest statement
S. Yano obtained grants from Chugai Pharma, Boehringer Ingelheim Japan, Novartis, and received speakers fees from AstraZeneca, Chugai Pharma, Boehringer Ingelheim Japan, Novartis, and Pfizer. T. Hase obtained grants from Boehringer Ingelheim Japan, AstraZeneca, Taiho Pharma, and Novartis, and received speakers fees from Boehringer Ingelheim Japan, Chugai Pharma, AstraZeneca, Ono Pharma, MSD, Bristol‐Myers Squibb, Taiho Pharma, Novartis, and travel support from Taiho Pharma, AstraZeneca, and Novartis. A. Hata obtained speakers fees and research grants from AstraZeneka, Taiho, Boehringer Ingelheim Japan, MSD, and Chugai Pharma. Y. Murakami obtained speakers fees from Taiho Pharma, Merck Sharp & Dohme, AstraZeneca, Chugai Pharma, Lilly Japan, Ono Pharma, Bristol‐Myers Squibb, Pfizer, Novartis, and Boehringer Ingelheim Japan, K. Yoshimura received speakers fees from Chugai Pharma, Astra Zeneca, and Eli Lilly. N. Katakami obtained speakers fees and research grants from AstraZeneka, Taiho, Boehringer Ingelheim Japan, MSD, and Chugai Pharma. T. Takahashi obtained grants from AstraZeneca, Chugai Pharma, Eli Lilly, Ono Pharma, MSD, and Pfizer, and received speakers fees from AstraZeneca, Chugai Pharma, Eli Lilly, from Ono Pharma, MSD, Pfizer, Boehringer Ingelheim Japan, and Roche Diagnostics. Y. Hasegawa obtained grants from AstraZeneca, Eli Lilly, Chugai Pharma, Ono Pharma, Novartis, Bristol‐Myers Squibb, and Taiho Pharma, and received speakers fees from AstraZeneca, Chugai Pharma, Boehringer Ingelheim Japan, MSD. and Pfizer. ST Ong obtained grants from the National Medical Research Council of Singapore (CSASI18may‐0004, NMRC/CSA/0051/2013, and NMRC/GMS/CIRG/1330/2012). The other authors have nothing to disclose.
Figures
Similar articles
-
Phase I study of combined therapy with vorinostat and gefitinib to treat BIM deletion polymorphism-associated resistance in EGFR-mutant lung cancer (VICTROY-J): a study protocol.J Med Invest. 2017;64(3.4):321-325. doi: 10.2152/jmi.64.321. J Med Invest. 2017. PMID: 28955007 Clinical Trial.
-
Histone Deacetylase 3 Inhibition Overcomes BIM Deletion Polymorphism-Mediated Osimertinib Resistance in EGFR-Mutant Lung Cancer.Clin Cancer Res. 2017 Jun 15;23(12):3139-3149. doi: 10.1158/1078-0432.CCR-16-2271. Epub 2016 Dec 16. Clin Cancer Res. 2017. PMID: 27986747
-
EGFR-TKI resistance due to BIM polymorphism can be circumvented in combination with HDAC inhibition.Cancer Res. 2013 Apr 15;73(8):2428-34. doi: 10.1158/0008-5472.CAN-12-3479. Epub 2013 Feb 4. Cancer Res. 2013. PMID: 23382048
-
BIM deletion polymorphism predicts poor response to EGFR-TKIs in nonsmall cell lung cancer: An updated meta-analysis.Medicine (Baltimore). 2019 Mar;98(10):e14568. doi: 10.1097/MD.0000000000014568. Medicine (Baltimore). 2019. PMID: 30855441 Free PMC article.
-
Optimizing the sequencing of tyrosine kinase inhibitors (TKIs) in epidermal growth factor receptor (EGFR) mutation-positive non-small cell lung cancer (NSCLC).Lung Cancer. 2019 Nov;137:113-122. doi: 10.1016/j.lungcan.2019.09.017. Epub 2019 Sep 23. Lung Cancer. 2019. PMID: 31568888 Free PMC article. Review.
Cited by
-
RNA splicing alterations in lung cancer pathogenesis and therapy.Cancer Pathog Ther. 2023 Apr 28;1(4):272-283. doi: 10.1016/j.cpt.2023.04.004. eCollection 2023 Oct. Cancer Pathog Ther. 2023. PMID: 38327600 Free PMC article. Review.
-
Histone Deacetylase Inhibition in Non-small Cell Lung Cancer: Hype or Hope?Front Cell Dev Biol. 2020 Oct 9;8:582370. doi: 10.3389/fcell.2020.582370. eCollection 2020. Front Cell Dev Biol. 2020. PMID: 33163495 Free PMC article. Review.
-
Targeting histone deacetylase enhances the therapeutic effect of Erastin-induced ferroptosis in EGFR-activating mutant lung adenocarcinoma.Transl Lung Cancer Res. 2021 Apr;10(4):1857-1872. doi: 10.21037/tlcr-21-303. Transl Lung Cancer Res. 2021. PMID: 34012798 Free PMC article.
-
Mechanisms of EGFR-TKI-Induced Apoptosis and Strategies Targeting Apoptosis in EGFR-Mutated Non-Small Cell Lung Cancer.Genes (Basel). 2022 Nov 22;13(12):2183. doi: 10.3390/genes13122183. Genes (Basel). 2022. PMID: 36553449 Free PMC article. Review.
-
Implications of Transglutaminase-Mediated Protein Serotonylation in the Epigenetic Landscape, Small Cell Lung Cancer, and Beyond.Cancers (Basel). 2023 Feb 20;15(4):1332. doi: 10.3390/cancers15041332. Cancers (Basel). 2023. PMID: 36831672 Free PMC article. Review.
References
-
- Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non‐small‐cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380‐2388. - PubMed
-
- Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non‐small‐cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol 2010;11:121‐128. - PubMed
-
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first‐line treatment for European patients with advanced EGFR mutation‐positive non‐small‐cell lung cancer (EURTAC): a multicentre, open‐label, randomised phase 3 trial. Lancet Oncol. 2012;13:239‐246. - PubMed
-
- Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327‐3334. - PubMed
-
- Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH. Osimertinib in untreated EGFR‐mutated advanced non‐small‐cell lung cancer. N Engl J Med. 2018;378:113‐125. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
