

Transanal endoscopic microsurgery for rectal villous tumours: Can we rely solely on preoperative biopsies and the surgeon’s experience?
- PMID: 31782642
- PMCID: PMC6877397
- DOI: 10.1503/cjs.012416
Transanal endoscopic microsurgery for rectal villous tumours: Can we rely solely on preoperative biopsies and the surgeon’s experience?
Abstract
Background: Transanal endoscopic microsurgery has become the standard of treatment for rectal villous adenomas. However, the role of preoperative imaging for these lesions is not clear. The aim of this study was to compare the value of preoperative imaging and surgeon clinical staging in the preoperative evaluation of patients with rectal villous adenomas having transanal endoscopic microsurgery resection.
Methods: We conducted a single-centre comparative retrospective cohort study of patients who underwent transanal endoscopic microsurgery surgery for rectal villous adenomas from 2011 to 2013. The intervention was preoperative imaging versus surgeon clinical staging. The primary outcome was the accuracy of clinical staging by preoperative imaging and surgeon clinical staging according to the histopathologic staging.
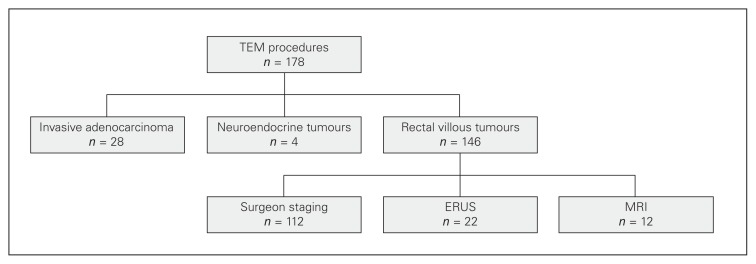
Results: A total of 146 patients underwent transanal endoscopic microsurgery surgery for rectal villous adenomas. One hundred and twelve (76.7%) of those patients had no preoperative imaging while 34 patients (23.3%) had either endorectal ultrasound (22 patients) or magnetic resonance imaging (12 patients). Surgeon staging was accurate in 89.3% of cases whereas staging by endorectal ultrasound was accurate in 40.9% cases and magnetic resonance imaging was accurate in 0% of cases. In the imaging group, inaccurate staging would have led to unnecessary radical surgery in 44.0% of patients.
Conclusion: This study was subject to selection bias because of its retrospective nature and the limited number of patients with imaging. Patients with rectal villous tumours without invasive carcinoma on biopsies and without malignant characteristics on appearance in the judgment of an experienced colorectal surgeon might not benefit from preoperative imaging before undergoing transanal endoscopic microsurgery procedures.
Contexte: La microchirurgie endoscopique transanale est devenue le traitement standard des adénomes villeux rectaux. La valeur de l’imagerie préopératoire pour le traitement de ces lésions n’est toutefois pas bien établie. Cette étude visait à comparer l’exactitude de la stadification par imagerie préopératoire et de la stadification clinique par le chirurgien dans le cadre de l’évaluation préopératoire des patients atteints d’adénomes villeux rectaux qui subissent une résection par microchirurgie endoscopique transanale.
Méthodes: Nous avons mené une étude de cohorte rétrospective comparative monocentrique chez des patients ayant subi une microchirurgie endoscopique transanale pour un adénome villeux rectal entre 2011 et 2013. Les interventions comparées étaient la stadification par imagerie préopératoire et la stadification clinique par le chirurgien. L’issue principale était l’exactitude de la stadification clinique par imagerie préopératoire et de la stadification clinique par le chirurgien, confirmée par stadification histopathologique.
Résultats: Au total, 146 patients ont subi une microchirurgie endoscopique transanale pour le traitement d’un adénome villeux rectal. De ces patients, 112 (76,7 %) n’avaient pas subi d’imagerie préopératoire et 34 (23,3 %) avaient subi une échographie endorectale (22 patients) ou une imagerie par résonance magnétique (12 patients). La stadification par le chirurgien était exacte dans 89,3 % des cas, contre 40,9 % des cas pour l’échographie endorectale et 0 % des cas pour l’imagerie par résonnance magnétique. Dans le groupe ayant subi une imagerie, l’inexactitude de la stadification aurait mené à une chirurgie radicale inutile pour 44,0 % des patients.
Conclusion: Cette étude comportait un biais de sélection en raison de sa nature rétrospective et du nombre limité de patients ayant subi une imagerie. L’imagerie préopératoire avant une microchirurgie endoscopique transanale pourrait ne présenter aucun avantage pour les patients présentant des tumeurs villeuses rectales dans les cas où aucun carcinome invasif n’a été détecté par biopsie et où un chirurgien colorectal chevronné n’a détecté aucune caractéristique maligne.
© 2019 Joule Inc. or its licensors
Conflict of interest statement
None declared.
Figures
Similar articles
-
Is magnetic resonance imaging useful for the management of patients with rectal villous adenoma? A study of 45 consecutive patients treated by transanal endoscopic microsurgery.Int J Colorectal Dis. 2018 Dec;33(12):1695-1701. doi: 10.1007/s00384-018-3148-x. Epub 2018 Aug 22. Int J Colorectal Dis. 2018. PMID: 30136172
-
Transanal endoscopic microsurgery: experience with 75 rectal neoplasms.Dis Colon Rectum. 2000 May;43(5):662-7; discussion 667-8. doi: 10.1007/BF02235583. Dis Colon Rectum. 2000. PMID: 10826428
-
Endorectal ultrasound detection of focal carcinoma within rectal adenomas.Am J Surg. 2004 May;187(5):625-9; discussion 629. doi: 10.1016/j.amjsurg.2004.01.005. Am J Surg. 2004. PMID: 15135679
-
[Treatment of rectal tumors with transanal endoscopic microsurgery].Medicina (Kaunas). 2005;41(6):470-6. Medicina (Kaunas). 2005. PMID: 15998984 Lithuanian.
-
Giant villous adenoma of rectum- what is the malignant potential and what is the optimal treatment? A case and review of literature.World J Surg Oncol. 2019 Jun 25;17(1):109. doi: 10.1186/s12957-019-1650-4. World J Surg Oncol. 2019. PMID: 31238922 Free PMC article. Review.
Cited by
-
Local full-thickness excision for sessile adenoma and cT1-2 rectal cancer: long-term oncological outcome.Langenbecks Arch Surg. 2022 Sep;407(6):2431-2439. doi: 10.1007/s00423-022-02593-7. Epub 2022 Jun 22. Langenbecks Arch Surg. 2022. PMID: 35732844 Free PMC article.
-
Analysis of the therapeutic effect of transanal endoscopic microsurgery on large rectal adenoma.J Minim Access Surg. 2022 Oct-Dec;18(4):571-577. doi: 10.4103/jmas.jmas_273_21. J Minim Access Surg. 2022. PMID: 36204937 Free PMC article.
-
The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience.J Clin Med. 2024 Feb 29;13(5):1419. doi: 10.3390/jcm13051419. J Clin Med. 2024. PMID: 38592246 Free PMC article.
References
-
- Jahadi MR, Baldwin A., Jr Villous adenomas of the colon and rectum. Am J Surg. 1975;130:729–32. - PubMed
-
- Cotran RS, Kumar V, Collins T. Robbins and Cotran pathologic basis of disease. 7th ed. New York (NY): Elsevier; 2006.
-
- Macciucca M, Casale A, Manganaro L, et al. Rectal villous tumors: MR features and correlation with TRUS in the preoperative evaluation. Eur J Radiol. 2010;73:329–33. - PubMed
-
- Heitman S, Ronksley P, Hilsden R, et al. Prevalence of adenomas and colorectal cancer in average risk individuals: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2009;7:1272–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources