

Beyond Margin Status: Population-Based Validation of the Proposed International Association for the Study of Lung Cancer Residual Tumor Classification Recategorization
- PMID: 31783180
- PMCID: PMC7044063
- DOI: 10.1016/j.jtho.2019.11.009
Beyond Margin Status: Population-Based Validation of the Proposed International Association for the Study of Lung Cancer Residual Tumor Classification Recategorization
Abstract
Introduction: The International Association for the Study of Lung Cancer's (IASLC's) proposal to recategorize the residual tumor (R) classification for resected NSCLC needs validation.
Methods: Using a 2009 to 2019 population-based multi-institutional NSCLC resection cohort from the United States, we classified resections by Union for International Cancer Control (UICC) and IASLC R criteria and compared the distribution of R classification variables and their survival associations.
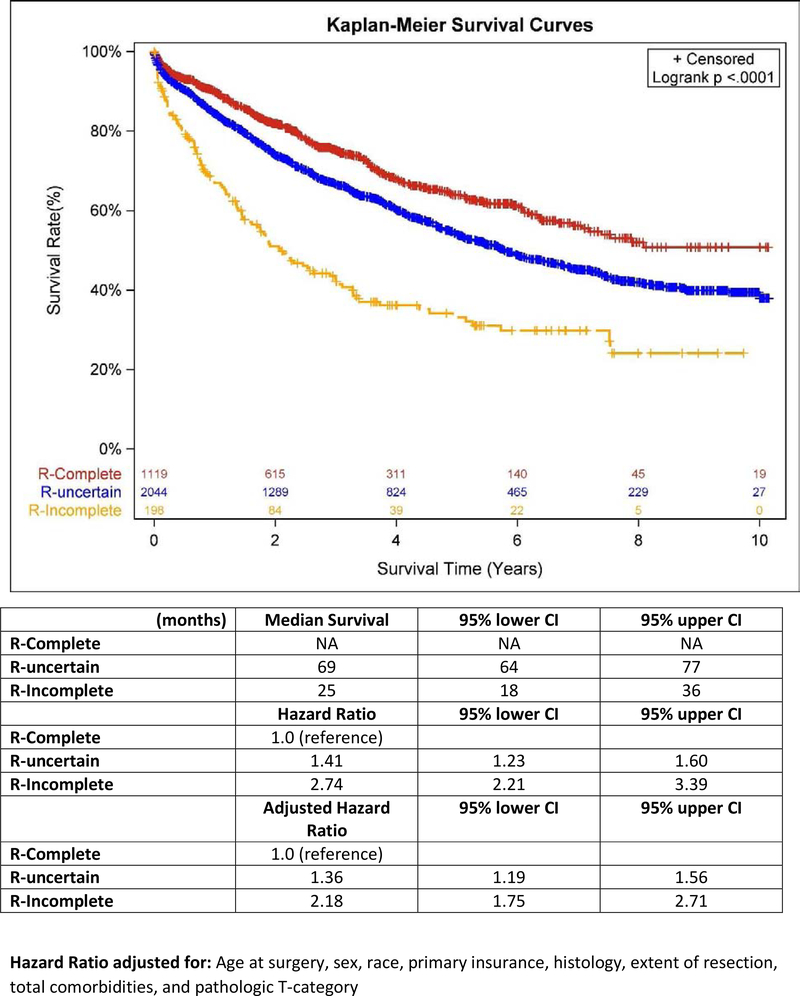
Results: Of 3361 resections, 95.3% were R0, 4.3% were R1, and 0.4% were R2 by UICC criteria; 33.3% were R0, 60.8% were R-uncertain, and 5.8% were R1/2 by IASLC criteria; 2044 patients (63.8%) migrated from UICC R0 to IASLC R-uncertain. Median survival was not reached, 69 (95% confidence interval [CI]: 64-77), and 25 (95% CI: 18-36) months, respectively, for patients with IASLC R0, R-uncertain, and R1 or R2 resections. Failure to achieve nodal dissection criteria caused 98% of migration to R-uncertainty, metastasis to the highest mediastinal node station, 5.8%. Compared with R0, R-uncertain resections with mediastinal nodes, no mediastinal nodes, and no nodes had adjusted hazard ratios of 1.28 (95% CI: 1.10-1.48), 1.47 (95% CI: 1.24-1.74), and 1.74 (95% CI: 1.37-2.21), respectively, suggesting a dose-response relationship between nodal R-uncertainty and survival. Accounting for mediastinal nodal involvement, the highest mediastinal station involvement was not independently prognostic. The incomplete resection variables were uniformly prognostic.
Conclusions: The proposed R classification recategorization variables were mostly prognostic, except the highest mediastinal nodal station involvement. Further categorization of R-uncertainty by severity of nodal quality deficit should be considered.
Keywords: Complete; Incomplete; Lung cancer; Lymph node; Resection margin; Staging.
Copyright © 2019 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures






References
-
- Kelsey CR, Marks LB, Hollis D, Hubbs JL, Ready NE, D’Amico TA, Boyd JA. Local recurrence after surgery for early stage lung cancer: an 11-year experience with 975 patients. Cancer. 2009. November 15;115(22):5218–27. - PubMed
-
- Purposes and principles of cancer staging In: Cancer Staging Handbook from the AJCC Cancer Staging Manual, 7th Edition. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (eds). Springer, NY, NY.
-
- Wind J, Smit EJ, Senan S, et al. Residual disease at the bronchial stump after curative resection for lung cancer. Eur J Cardiothorac Surg 2007;32(1):29–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
