

Risk factors of neurological deficit and pulmonary cement embolism after percutaneous vertebroplasty
- PMID: 31783861
- PMCID: PMC6884871
- DOI: 10.1186/s13018-019-1459-4
Risk factors of neurological deficit and pulmonary cement embolism after percutaneous vertebroplasty
Abstract
Background: The risk factors, incidence, and clinical management of pulmonary cement embolism and neurological deficit during percutaneous vertebroplasty (PVP) were evaluated.
Methods: Three thousand one hundred and seventy-five patients with symptomatic osteoporotic vertebral compression fractures (OVCFs) treated with PVP were retrospectively reviewed in a single institution. Clinical parameters such as age, gender, number of fractures, and time from fracture to vertebroplasty were recorded at the time of surgery. Image and surgical parameters including the amount of cement, the vertebral level, uni- or bipedicle surgical approach, and leakage pattern were recorded.
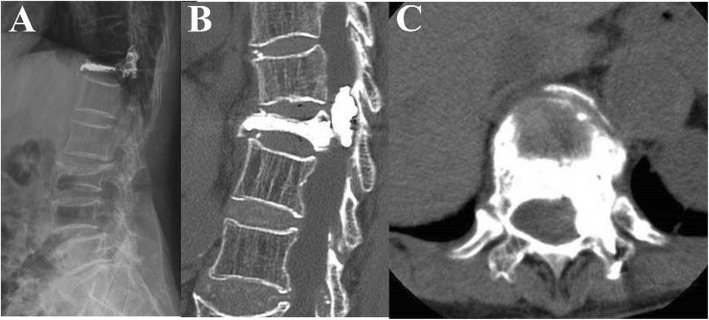
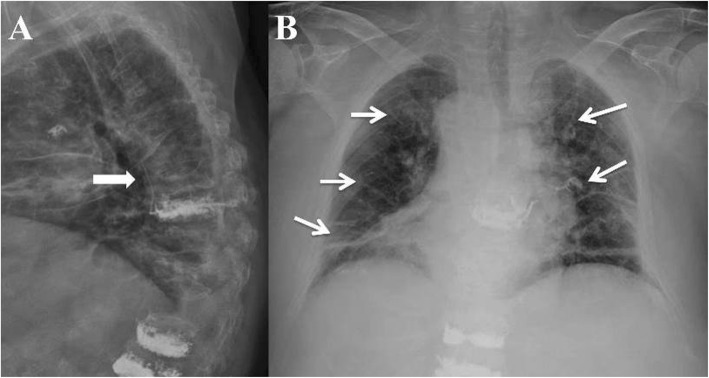
Results: Type-C leakage, including paraspinal (25%), intradiscal (26%), and posterior (0.7%) leakage, was more common than type-B (11.4%) and type-S leaks (4.9%). Cement leakage into the spinal canal (type-C posterior) occurred in 26 patients (0.7%), and four patients needed surgical decompression. Three in nine patients with leakage into thoracic spine needed decompressive surgery, but only one of 17 patients into lumbar spine needed surgery (p < 0.01). Age, gender, number of fractures, and time from fracture to vertebroplasty were not risk factors of pulmonary cement embolism or neurological deficit. The risk factor of pulmonary cement embolism was higher volume of PMMA injected (p < 0.001) and risk factor of neurological deficit was type-C posterior cement leakage into thoracic spine. The incidence of pulmonary cement embolism was significantly high in the volume of PMMA injected (PMMA injection < 3.5 cc: 0%; 3.5-7.0 cc: 0.11%; > 7.0 cc: 0.9%; p < 0.01) which needed postoperative oxygen support.
Conclusions: Cement leakage is relatively common but mostly of no clinical significance. Percutaneous vertebroplasty in thoracic spine and high amount of PMMA injected should be treated with caution in clinical practice.
Keywords: Adverse effects; Bone cements; Iatrogenic disease; Paresis; Pulmonary embolism.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hussain A, Erdek M. Vertebroplasty augmentation procedures: examining the controversy. Pain Physician. 2013;16:E483–E490. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
