

Trends in horizontal inequity in access to public health care services by immigrant condition in Spain (2006-2017)
- PMID: 31783864
- PMCID: PMC6883664
- DOI: 10.1186/s12939-019-1092-1
Trends in horizontal inequity in access to public health care services by immigrant condition in Spain (2006-2017)
Abstract
Background: The objective of this research is to analyse trends in horizontal inequity in access to public health services by immigration condition in Spain throughout the period 2006-2017. We focus on "economic immigrants" because they are potentially the most vulnerable group amongst immigrants.
Methods: Based on the National Health Surveys of 2006-07 (N = 29,478), 2011-12 (N = 20,884) and 2016-17 (N = 22,903), hierarchical logistic regressions with random effects in Spain's autonomous communities are estimated to explain the probability of using publicly-financed health care services by immigrant condition, controlling by health care need and other socioeconomic and demographic variables.
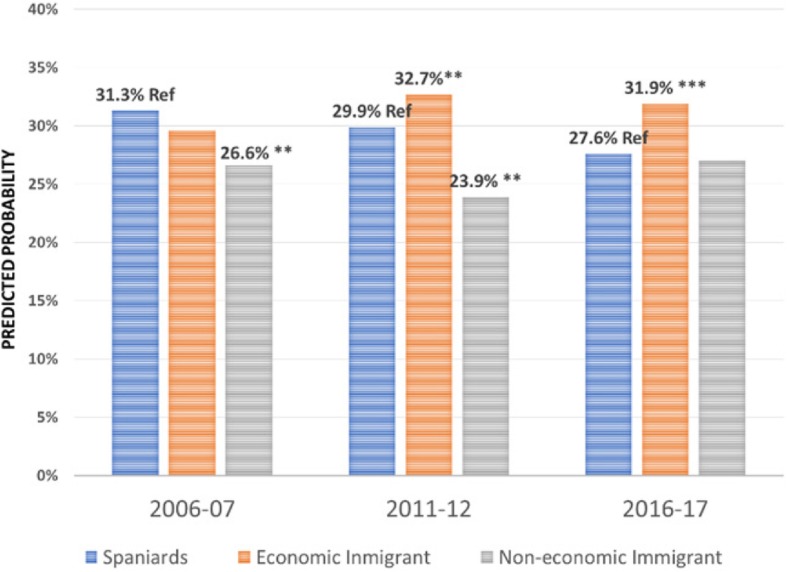
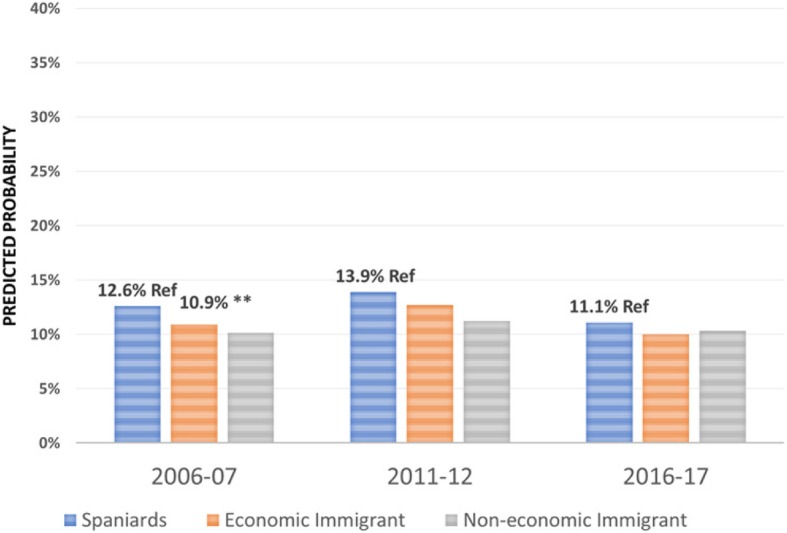
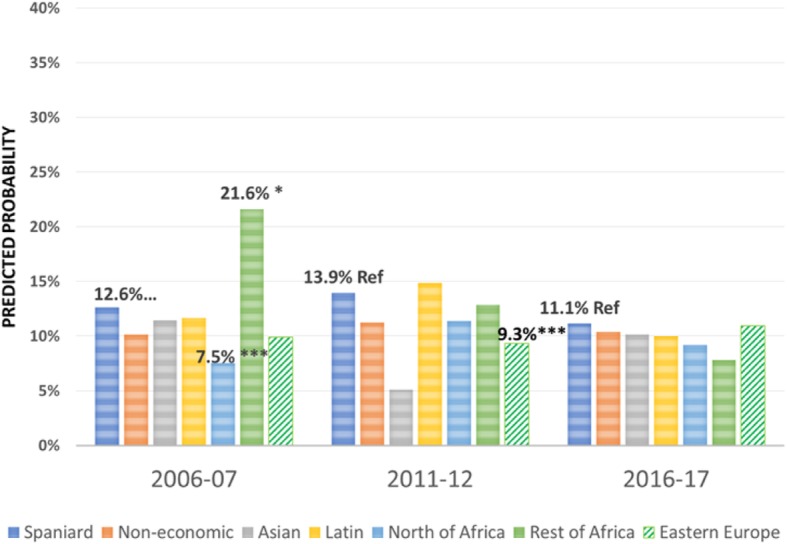
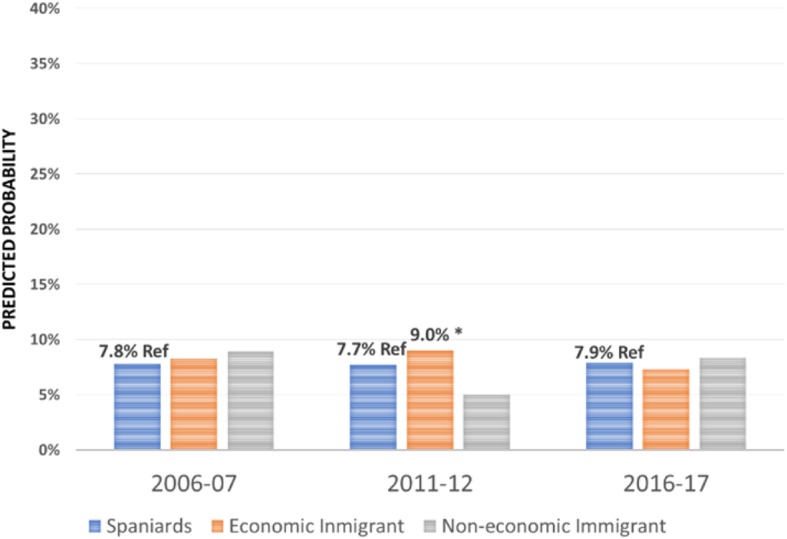
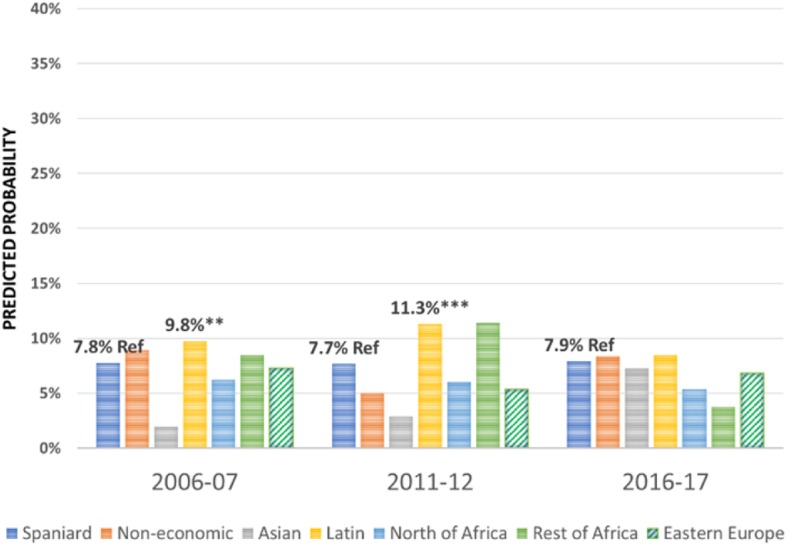
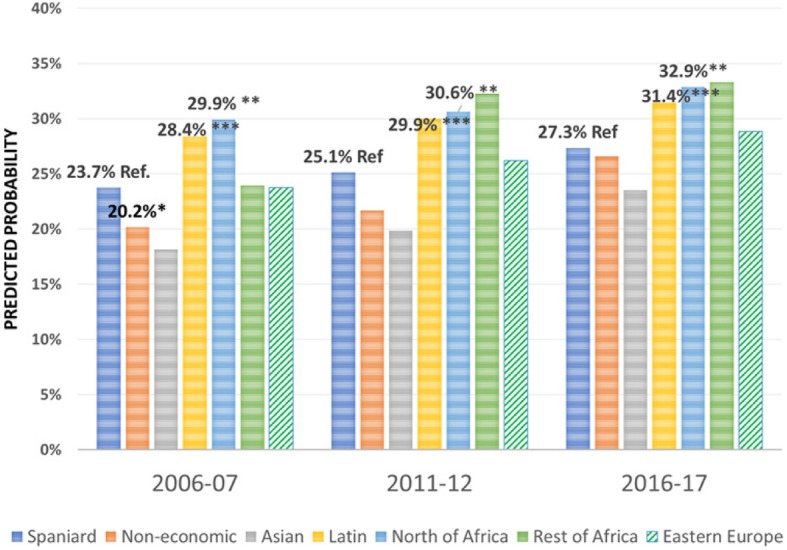
Results: Our results indicate that there are several horizontal inequities, though they changed throughout the decade studied. Regarding primary care services, the period starts (2006-07) with no global evidence of horizontal inequity in access (although the analysis by continent shows inequity that is detrimental to Eastern Europeans and Asians), giving way to inequity favouring economic immigrants (particularly Latin Americans and Africans) in 2011-12 and 2016-17. An opposite trend happens with specialist care, as the period starts (2006-07) with evidence of inequity that is detrimental to economic immigrants (particularly those from North of Africa) but this inequity disappears with the economic crisis and after it (with the only exception of Eastern Europeans in 2011-12, whose probability to visit a specialist is lower than for natives). Regarding emergency care, our evidence indicates horizontal inequity in access that favours economic immigrants (particularly Latin Americans and North Africans) that remains throughout the period. In general, there is no inequity in hospitalisations, with the exception of 2011-12, where inequity in favour of economic immigrants (particularly those from Latin America) takes place.
Conclusions: The results obtained here may serve, firstly, to prevent alarm about negative discrimination of economic immigrants in their access to public health services, even after the implementation of the Royal Decree RD Law 16/2012. Conversely, our results suggest that the horizontal inequity in access to specialist care that was found to be detrimental to economic immigrants in 2006-07, disappeared in global terms in 2011-12 and also by continent of origin in 2016-17.
Keywords: Economic immigration; Horizontal equity in access; National health surveys; Public health care services.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Factors determining access to and use of primary health care services in the Girona Health Region (Spain).Eur J Health Econ. 2012 Aug;13(4):419-27. doi: 10.1007/s10198-011-0313-3. Epub 2011 Apr 16. Eur J Health Econ. 2012. PMID: 21499790
-
Horizontal equity in access to public GP services by socioeconomic group: potential bias due to a compartmentalised approach.Int J Equity Health. 2019 Dec 2;18(1):187. doi: 10.1186/s12939-019-1091-2. Int J Equity Health. 2019. PMID: 31791347 Free PMC article.
-
Understanding differences in access and use of healthcare between international immigrants to Chile and the Chilean-born: a repeated cross-sectional population-based study in Chile.Int J Equity Health. 2012 Nov 16;11:68. doi: 10.1186/1475-9276-11-68. Int J Equity Health. 2012. PMID: 23158113 Free PMC article.
-
Why is the 'healthy immigrant effect' different between European countries?Eur J Public Health. 2014 Aug;24 Suppl 1:80-6. doi: 10.1093/eurpub/cku112. Eur J Public Health. 2014. PMID: 25108002 Review.
-
[Immigrants' access to health care in Spain: a review].Rev Esp Salud Publica. 2014 Nov-Dec;88(6):715-34. doi: 10.4321/S1135-57272014000600005. Rev Esp Salud Publica. 2014. PMID: 25418563 Review. Spanish.
Cited by
-
Unequal nursing: the impact of China's public health insurance on nursing services for older adults.BMC Nurs. 2025 Jul 1;24(1):803. doi: 10.1186/s12912-025-03459-1. BMC Nurs. 2025. PMID: 40597215 Free PMC article.
References
-
- Hernández-Quevedo C, Jiménez-Rubio D. A comparison of the health status and health care utilization patterns between foreigners and the national population in Spain: new evidence from the Spanish national health survey. Soc Sci Med. 2009;69:370–378. doi: 10.1016/j.socscimed.2009.05.005. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
