

The Usefulness of Lung Ultrasound for the Aetiological Diagnosis of Community-Acquired Pneumonia in Children
- PMID: 31784642
- PMCID: PMC6884636
- DOI: 10.1038/s41598-019-54499-y
The Usefulness of Lung Ultrasound for the Aetiological Diagnosis of Community-Acquired Pneumonia in Children
Abstract
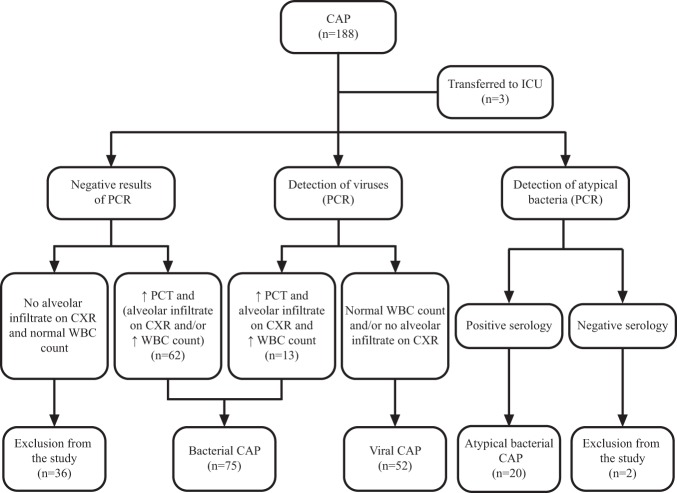
The aetiology of community-acquired pneumonia (CAP) is not easy to establish. As lung ultrasound (LUS) has already proved to be an excellent diagnostic tool for CAP, we analysed its usefulness for discriminating between the aetiologically different types of CAP in children. We included 147 children hospitalized because of CAP. LUS was performed in all patients at admission, and follow-up LUS was performed in most patients. LUS-detected consolidations in viral CAP were significantly smaller, with a median diameter of 15 mm, compared to 20 mm in atypical bacterial CAP (p = 0.05) and 30 mm in bacterial CAP (p < 0.001). Multiple consolidations were detected in 65.4% of patients with viral CAP and in 17.3% of patients with bacterial CAP (p < 0.001). Bilateral consolidations were also more common in viral CAP than in bacterial CAP (51.9% vs. 8.0%, p < 0.001). At follow-up, a regression of consolidations was observed in 96.6% of patients with bacterial CAP and in 33.3% of patients with viral CAP (p < 0.001). We found LUS to be especially suitable for differentiating bacterial CAP from CAP due to other aetiologies. However, LUS must be interpreted in light of clinical and laboratory findings.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
