

Efficacy and safety of subthreshold micropulse laser compared with threshold conventional laser in central serous chorioretinopathy
- PMID: 31784704
- PMCID: PMC7608089
- DOI: 10.1038/s41433-019-0692-8
Efficacy and safety of subthreshold micropulse laser compared with threshold conventional laser in central serous chorioretinopathy
Abstract
Purpose: To compare the efficacy and safety of subthreshold micropulse laser (SML) with threshold conventional laser (TCL) in central serous chorioretinopathy (CSC).
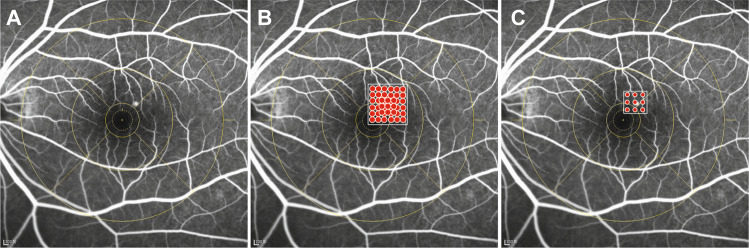
Methods: Prospective, randomized, double-masked, non-inferiority, 12-week clinical trial. Patients were randomly assigned 1:1 to SML group or TCL group. Patients in the SML group were treated with 577 nm micropulse laser. The spot size was 160 µm, the duty cycle was 5% and exposure time was 0.2 s. The power was 50% threshold tested. Patients in the TCL group were treated with 577 nm continuous laser. The power was 100% threshold tested. The primary outcome was the mean change in best-corrected visual acuity (BCVA) at week 12, with a non-inferiority limit of five letters on the Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity charts.
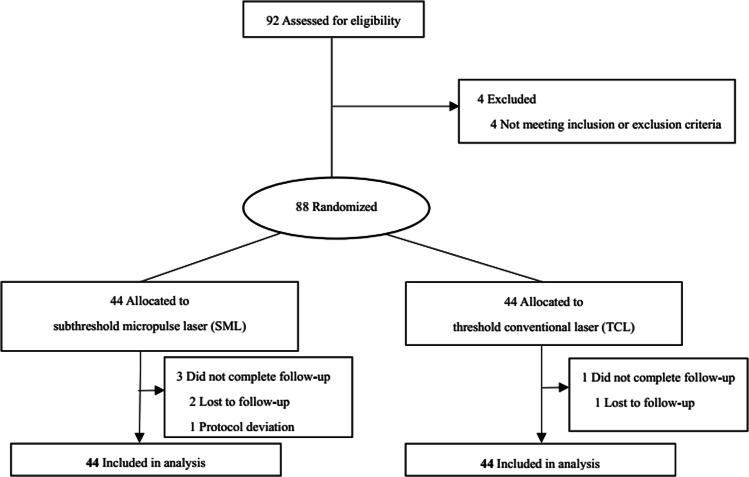
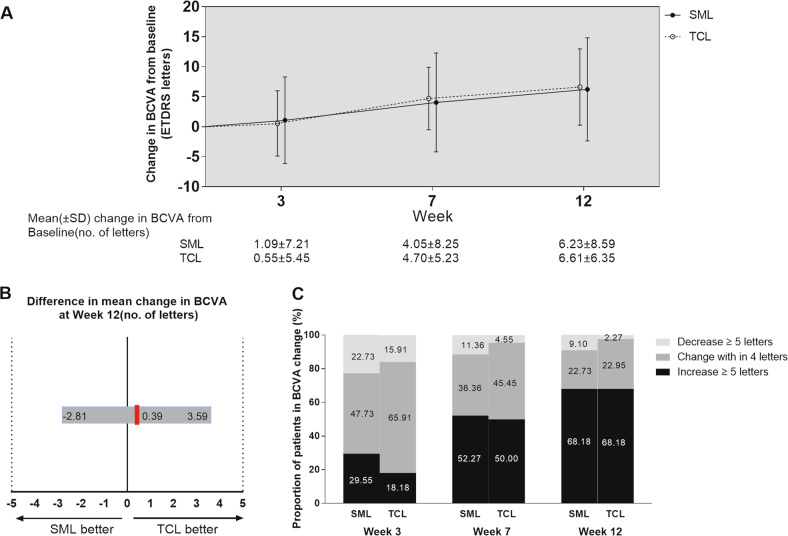
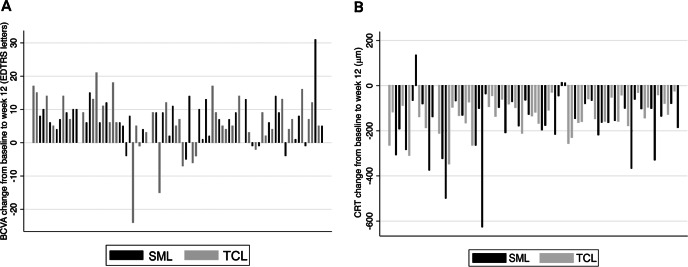
Results: Eighty-eight patients were enroled. Seventy-seven patients were male. Forty-four patients were in SML group and 44 in TCL group. At week 12, SML was equivalent to TCL with a gain of 6.23 ± 8.59 and 6.61 ± 6.35 letters, respectively, (SML-TCL difference: -0.38 letters; 95% confidence interval (CI):-3.58-2.81; Pnon-inferiority = 0.0026). There was no statistically significant difference between the two groups (t = 0.240, P = 0.811). At week 12, the proportion of patients whose SRF had been totally absorbed was 63.63 and 81.82% respectively for SML and TCL groups. There was no statistically significant difference between the two groups (χ2 = 3.67, P = 0.056).
Conclusions: Both SML and TCL can improve visual acuity in CSC. SML was non-inferior to TCL in the improvement of BCVA.
Conflict of interest statement
Victor Chong is a consultant for Quantel Medical. The other authors declare that they have no conflict of interest.
Figures
Comment in
-
Correspondence on: Efficacy and safety of subthreshold micropulse laser compared with threshold conventional laser in central serous chorioretinopathy.Eye (Lond). 2021 Nov;35(11):3161-3162. doi: 10.1038/s41433-020-01253-8. Epub 2020 Oct 29. Eye (Lond). 2021. PMID: 33122848 Free PMC article. No abstract available.
References
-
- Palanker D, Blumenkranz MS. Retinal laser therapy: biophysical basisand applications. In: Ryan S, Wilkinson H, Sadda W, editors. Ch. 39. RETINA. 5th ed. Vol. 1. Elsevier Inc; 2013, p. 752–5.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
