

The contribution of frailty, cognition, activity of daily life and comorbidities on outcome in acutely admitted patients over 80 years in European ICUs: the VIP2 study
- PMID: 31784798
- PMCID: PMC7223711
- DOI: 10.1007/s00134-019-05853-1
The contribution of frailty, cognition, activity of daily life and comorbidities on outcome in acutely admitted patients over 80 years in European ICUs: the VIP2 study
Abstract
Purpose: Premorbid conditions affect prognosis of acutely-ill aged patients. Several lines of evidence suggest geriatric syndromes need to be assessed but little is known on their relative effect on the 30-day survival after ICU admission. The primary aim of this study was to describe the prevalence of frailty, cognition decline and activity of daily life in addition to the presence of comorbidity and polypharmacy and to assess their influence on 30-day survival.
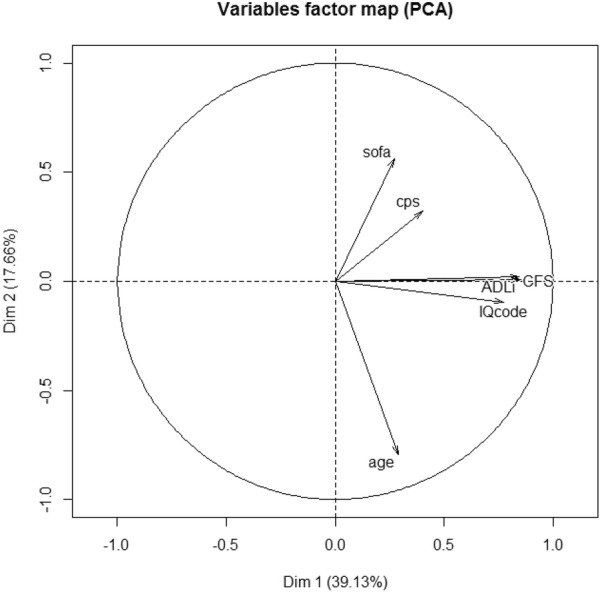
Methods: Prospective cohort study with 242 ICUs from 22 countries. Patients 80 years or above acutely admitted over a six months period to an ICU between May 2018 and May 2019 were included. In addition to common patients' characteristics and disease severity, we collected information on specific geriatric syndromes as potential predictive factors for 30-day survival, frailty (Clinical Frailty scale) with a CFS > 4 defining frail patients, cognitive impairment (informant questionnaire on cognitive decline in the elderly (IQCODE) with IQCODE ≥ 3.5 defining cognitive decline, and disability (measured the activity of daily life with the Katz index) with ADL ≤ 4 defining disability. A Principal Component Analysis to identify co-linearity between geriatric syndromes was performed and from this a multivariable model was built with all geriatric information or only one: CFS, IQCODE or ADL. Akaike's information criterion across imputations was used to evaluate the goodness of fit of our models.
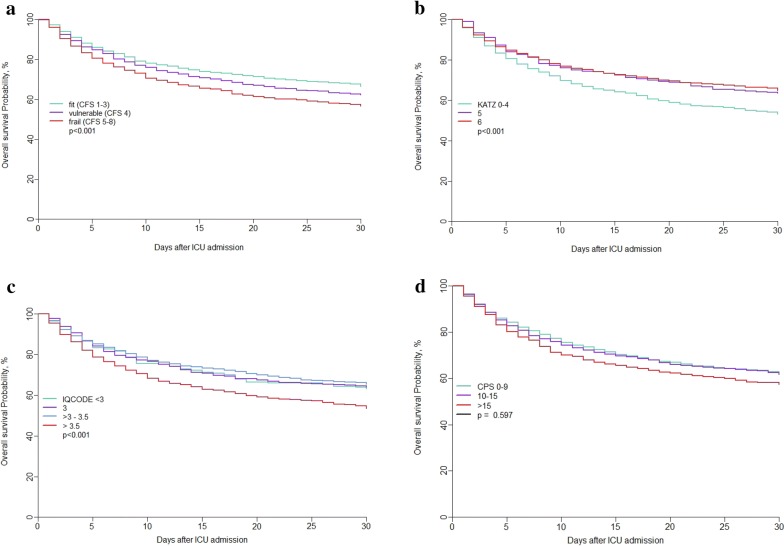
Results: We included 3920 patients with a median age of 84 years (IQR: 81-87), 53.3% males). 80% received at least one organ support. The median ICU length of stay was 3.88 days (IQR: 1.83-8). The ICU and 30-day survival were 72.5% and 61.2% respectively. The geriatric conditions were median (IQR): CFS: 4 (3-6); IQCODE: 3.19 (3-3.69); ADL: 6 (4-6); Comorbidity and Polypharmacy score (CPS): 10 (7-14). CFS, ADL and IQCODE were closely correlated. The multivariable analysis identified predictors of 1-month mortality (HR; 95% CI): Age (per 1 year increase): 1.02 (1.-1.03, p = 0.01), ICU admission diagnosis, sequential organ failure assessment score (SOFA) (per point): 1.15 (1.14-1.17, p < 0.0001) and CFS (per point): 1.1 (1.05-1.15, p < 0.001). CFS remained an independent factor after inclusion of life-sustaining treatment limitation in the model.
Conclusion: We confirm that frailty assessment using the CFS is able to predict short-term mortality in elderly patients admitted to ICU. Other geriatric syndromes do not add improvement to the prediction model. Since CFS is easy to measure, it should be routinely collected for all elderly ICU patients in particular in connection to advance care plans, and should be used in decision making.
Keywords: Activities of daily living; Cognitive functioning; Comorbidity; Critical care; Elderly; Frailty; Outcome; Prediction.
Conflict of interest statement
Joerg C. Schefold declares that the Dept. of Intensive Care Medicine Bern has/had research and/or development/consulting contracts with (full disclosure): Orion Corporation, Abbott Nutrition International, B. Braun Medical AG, CSEM SA, Edwards Lifesciences Services GmbH/SA, Kenta Biotech Ltd, Maquet Critical Care AB, Omnicare Clinical Research AG, and Nestlé. Educational grants were received from Fresenius Kabi; GSK; MSD; Lilly; Baxter; Astellas; AstraZeneca; B. Braun Medical AG, CSL Behring, Maquet, Novartis, Covidien, Nycomed, Pierre Fabre Pharma (Roba Pharma); Pfizer, Orion Pharma. The money went into departmental funds. No personal financial gain applies. All other authors do not have any conflict of interest to declare related to this manuscript.
Figures
Comment in
-
Frailty and unplanned admissions to the intensive care unit: a retrospective cohort study in the UK.Intensive Care Med. 2020 Jul;46(7):1512-1513. doi: 10.1007/s00134-020-06020-7. Epub 2020 Apr 2. Intensive Care Med. 2020. PMID: 32240348 No abstract available.
-
Frailty assessment in very old intensive care patients: the Hospital Frailty Risk Score answers another question.Intensive Care Med. 2020 Jul;46(7):1514-1515. doi: 10.1007/s00134-020-06095-2. Epub 2020 May 25. Intensive Care Med. 2020. PMID: 32451580 Free PMC article. No abstract available.
-
Frailty assessment in very old intensive care patients: the Hospital Frailty Risk Score answers another question.Intensive Care Med. 2020 Jul;46(7):1516-1517. doi: 10.1007/s00134-020-06107-1. Epub 2020 May 27. Intensive Care Med. 2020. PMID: 32462325 No abstract available.
References
-
- Margaras V (2019) Demographic trends in EU regions. European Parliamentary Research Service, January 2019. https://ec.europa.eu/futurium/en/system/files/ged/eprs-briefing-633160-d...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
