

B Cell Synovitis and Clinical Phenotypes in Rheumatoid Arthritis: Relationship to Disease Stages and Drug Exposure
- PMID: 31785084
- PMCID: PMC7217046
- DOI: 10.1002/art.41184
B Cell Synovitis and Clinical Phenotypes in Rheumatoid Arthritis: Relationship to Disease Stages and Drug Exposure
Abstract
Objective: To define the relationship of synovial B cells to clinical phenotypes at different stages of disease evolution and drug exposure in rheumatoid arthritis (RA).
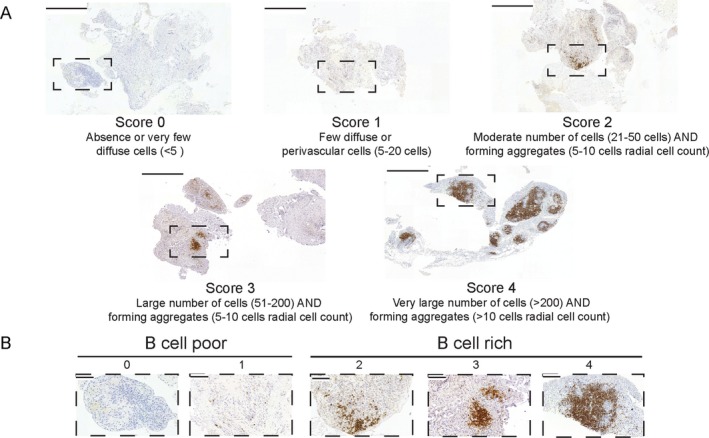
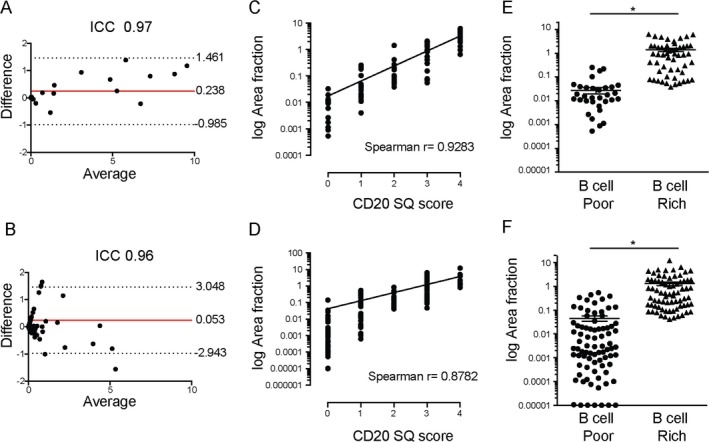
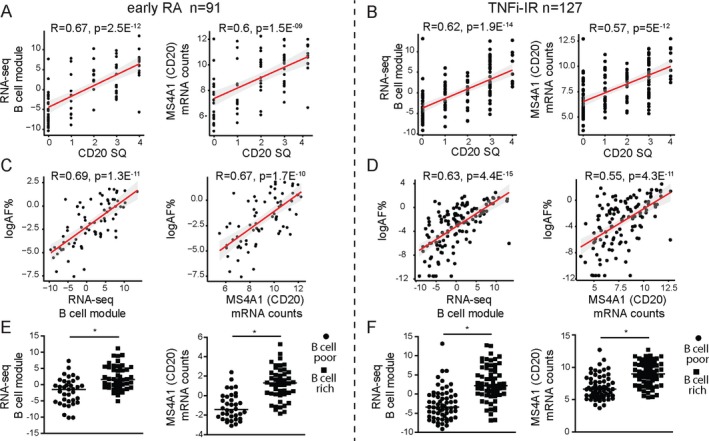
Methods: Synovial biopsy specimens and demographic and clinical data were collected from 2 RA cohorts (n = 329), one of patients with untreated early RA (n = 165) and one of patients with established RA with an inadequate response to tumor necrosis factor inhibitors (TNFi-IR; n = 164). Synovial tissue was subjected to hematoxylin and eosin and immunohistochemical staining and semiquantitative assessment for the degree of synovitis (on a scale of 0-9) and of CD20+ B cell infiltrate (on a scale of 0-4). B cell scores were validated by digital image analysis and B cell lineage-specific transcript analysis (RNA-Seq) in the early RA (n = 91) and TNFi-IR (n = 127) cohorts. Semiquantitative CD20 scores were used to classify patients as B cell rich (≥2) or B cell poor (<2).
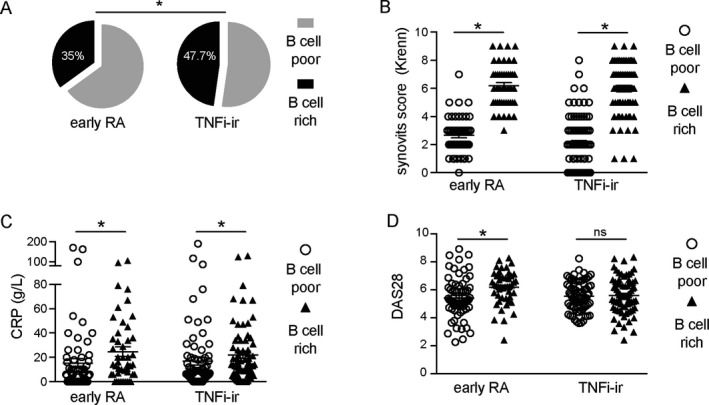
Results: Semiquantitative B cell scores correlated with digital image analysis quantitative measurements and B cell lineage-specific transcripts. B cell-rich synovitis was present in 35% of patients in the early RA cohort and 47.7% of patients in the TNFi-IR cohort (P = 0.025). B cell-rich patients showed higher levels of disease activity and seropositivity for rheumatoid factor and anti-citrullinated protein antibody in early RA but not in established RA, while significantly higher histologic synovitis scores in B cell-rich patients were demonstrated in both cohorts.
Conclusion: We describe a robust semiquantitative histologic B cell score that closely replicates the quantification of B cells by digital or molecular analyses. Our findings indicate an ongoing B cell-rich synovitis, which does not seem to be captured by standard clinimetric assessment, in a larger proportion of patients with established RA than early RA.
© 2019 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
Comment in
-
Advancing Rheumatoid Arthritis Synovial Biopsy Analysis: One B Cell at a Time.Arthritis Rheumatol. 2020 May;72(5):702-703. doi: 10.1002/art.41185. Epub 2020 Mar 23. Arthritis Rheumatol. 2020. PMID: 31785078 Free PMC article. No abstract available.
References
-
- Edwards JC, Szczepański L, Szechiński J, Filipowicz‐Sosnowska A, Emery P, Close DR, et al. Efficacy of B‐cell–targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med 2004;350:2572–81. - PubMed
-
- Kramm H, Hansen KE, Gowing E, Bridges A. Successful therapy of rheumatoid arthritis with rituximab: renewed interest in the role of B cells in the pathogenesis of rheumatoid arthritis. J Clin Rheumatol 2004;10:28–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
